
The Truth about VO2max: what it is and why it matters

VO2max has hit the headlines because a lot of people have noticed a mismatch between what metric the strongest long term datasets linking cardiorespiratory fitness and mortality actually measured, METs, and what the public conversation thinks they measured, VO2max.
Much of the data for these big studies assessing cardiorespiratory fitness comes from treadmill tests reported in METs, not VO2max from breath by breath gas analysis. At the same time, consumer devices have started pushing VO2max estimates as if they were a clinical grade assessment. That combination has created a predictable backlash.

I understand the frustration. If you turn VO2max into a longevity badge, people will chase it, at the detriment of other similarly important aspects of health and fitness such as resistance training, mobility and stability. If a watch can estimate it (with a significant meaningful error), people will treat small week to week changes as real. If clinicians then respond to a shaky estimate with more testing, you end up optimising for a number that has drifted several steps away from the underlying physiology. The argument should not be anti VO2max. It is anti abstraction.
It is easy to miss the real culprit. The problem is not VO2max as a physiological concept. The problem is the method used to generate the number, and what we try to do with it. Directly measured VO2 from a properly run cardiopulmonary exercise test tells you far more than a headline score. It is diagnostic, prognostic and prescriptive. It gives you a map of limitations and a basis for personalised training prescription. If we let poor estimation and poor interpretation discredit the whole construct, we lose one of the most useful ways to quantify cardiorespiratory fitness, and we lose the clinical value that comes with measuring it well.
In this article, I explain the differences in these metrics, why they are important and where people have become unstuck.
Start with the thing we actually care about: cardiorespiratory fitness
Cardiorespiratory fitness (CRF) is the underlying physiology that we are interested in and is what may often be referred to as athletic fitness. It is a measure of how well our cardiovascular, respiratory and metabolic systems interact with each other and thus, one of the few metrics that represent a whole-systems assessment of how well these systems are functioning.
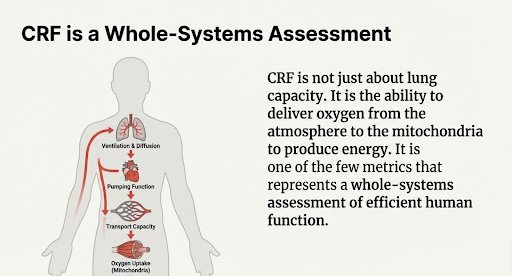
It is your ability to deliver oxygen to working muscle and use it to produce energy. For a system to function efficiently means transporting oxygen from the atmosphere through to the mitochondria in your muscles in order for physical activity to be performed. It is a thorough quantification of and dependent on:
Your lung ventilation and diffusion of gases into the blood stream
Heart function
Capacity of your blood vessels to accommodate and transport blood from the heart to the muscles
Ability to precisely match the oxygen delivery to oxygen demand
Ability of the muscles to take up and utilise oxygen and nutrients transported by blood
Communication of these cardiovascular and metabolic demands to the cardiovascular control centre
Leaving the intricacies of medical diagnostics aside, I’ll discuss the prognostic implications.
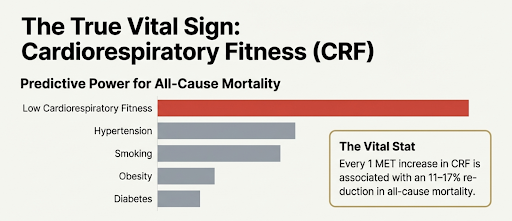
CRF matters because it is strongly linked to health outcomes. The American Heart Association has argued that CRF deserves “vital sign” status in clinical practice because low CRF consistently associates with higher risk of cardiovascular disease and all cause mortality [1]. One of the most recent meta-analyses (looking at studies reported in MET and VO2max), spanning 20.9 million observations found that every 1 MET higher level of CRF was associated with a 11-17% reduction in all-cause mortality [2].
It is one of the best predictors of:
Overall risk of death [2]
Cardiovascular mortality [3]
Cancer mortality [4]
Incidence of diabetes, high blood pressure, stroke, dementia, kidney disease, depression, and much more [2]
Better cognitive performance in middle age [5], later onset of dementia and a 35% reduction in risk in those with a moderate/high polygenic risk of dementia [6].
CRF has been demonstrated to be a more powerful predictor of risk of death than the more traditional risk factors such as hypertension, diabetes, obesity, hyperlipidaemia and smoking [1].
CRF can be measured in several ways. In research studies, two commonly reported units VO2max and METs.
VO2max versus METs
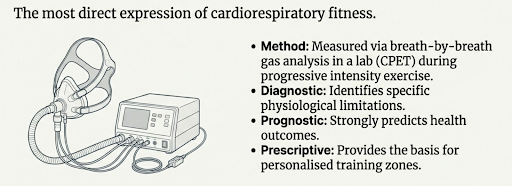
VO₂max is the most direct expression of cardiorespiratory fitness. This essentially measures highest rate that your tissues and muscles take up oxygen during progressive intensive treadmill or cycling test, captured in a lab using breath by breath gas analysis in a cardiopulmonary exercise test.
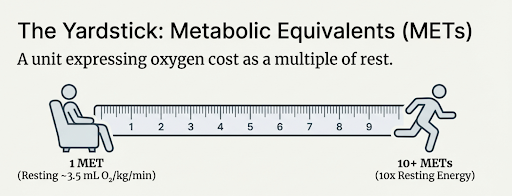
METs are not a different biological process. A MET, or metabolic equivalent, is a unit that expresses oxygen cost as a multiple of rest, with 1 MET conventionally defined as 3.5 mL O₂ per kg per minute, roughly the oxygen consumption of sitting quietly [3]. They are a way of expressing oxygen cost as multiples of resting metabolism.
You can convert a directly measured VO₂ value into METs by dividing by 3.5. But when METs come from treadmill speed and incline tables, they are only an estimate of oxygen uptake, not a direct measurement, and they carry more individual level error.
That convenience is exactly why METs show up everywhere in research and clinical reports. They let you compare workloads across protocols and modalities of exercise. It is cheaper to measure and simpler. They let you standardise outcomes across large cohorts.
But the key point is that METs are not a different physiological construct from VO2. They are a way of expressing oxygen uptake, or estimated oxygen uptake, in a standardised unit.
1 MET is not “one size fits all”
The 3.5 value is a convention, not your personal resting metabolic rate.
Resting oxygen consumption varies with sex, age, body composition, pregnancy status, and training status. A paper that directly tested the 1 MET assumption across different groups showed meaningful mismatch between the standard value and measured resting metabolic rate [7].
This doesn’t mean METs are wrong but it does mean you should treat METs as useful approximations, not precision assessments for individuals.
What went wrong reporting the big studies?
In the longevity field, several papers are commonly cited such as Mandsager [8], Kokkinos [9] and the Kodama [10]. These analyses standardise cardiorespiratory fitness expressed as METs, though some of the primary papers included VO2 based testing [7].
Some have used this literature to claim that VO2max is the single most powerful metric that predicts how long you will live, when much of the underpinning evidence actually reports fitness in MET units.
The core issue is method, not meaning. Many of the largest cohorts did not measure oxygen uptake directly. They estimated exercise capacity from treadmill workload and expressed it in METs. That is still cardiorespiratory fitness. It is still aerobic capacity. But it is not technically the same as a lab measured VO2max from gas exchange.
This is also why pooled analyses need standardisation. Meta analyses that include both directly measured VO2 and indirect exercise estimated fitness have to convert results into a common unit. METs provide that common language. So when a study reports that each 1 MET higher fitness associates with lower mortality, it is still tracking aerobic capacity. The unit is standardised. The measurement method behind the unit varies.
Importantly, the signal does not vanish when you compare methods. A more recent systematic review and meta analysis of 42 studies and 3.8 million observations compared objectively measured fitness, exercise estimated fitness, and non exercise estimated fitness, and found similar risk reductions per stepped increment in cardiorespiratory fitness [3]. So the problem is not that MET based evidence is weaker. The problem is that people collapse distinct measurement approaches into one headline term, then build further abstraction on top of that. That does not mean VO2 measurement is irrelevant. It means estimated CRF is often “good enough” for ranking risk across populations.
Once you do that, it becomes easy to mistake a convenient consumer estimate for a clinical measurement. That is where the real risk sits. Not in VO2max as a physiological construct, but in treating a noisy estimate as if it carries the same meaning as a properly conducted cardiopulmonary exercise test.
Wearable VO2 estimates: useful direction, limited precision
Wearables can estimate VO2max using rest data, exercise data, or both.
At the population level, some of the data look acceptable. At the individual level, the error can be significant. The INTERLIVE systematic review and meta analysis found wide limits of agreement, even when average bias looked small. That is the scenario where people overinterpret their figures month to month and make unwarranted conclusions and adjustments to their training.
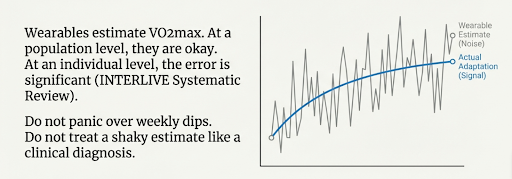
Use wearables for behaviour feedback and broad direction.
Do not use them to diagnose problems or to panic over minor dips.
Why CPET becomes more valuable at the individual level
Population research asks: “Who is at higher risk?”
Individual care asks: “Why is this person limited, and what should they do next?”
VO2peak or VO2max is only one output from a cardiorespiratory fitness test. As highlighted earlier, it is a whole-systems measure of lung, heart and muscular function. This is precisely why it a CPET is so useful. One CPET gives you VO2max, plus 20 plus additional, clinically useful metrics for diagnosis prognosis and prescription of a personalised training programme.
The exact list varies by device and protocol, but you typically get 20 to 30 interpretable variables and other metrics.
Aside from the prognostic factors above, it can separate common limiting physiological issues, be that the heart function or physiology, dysfunctional breathing, the exchange of gas from the lungs to the blood, issues in the muscle and more.
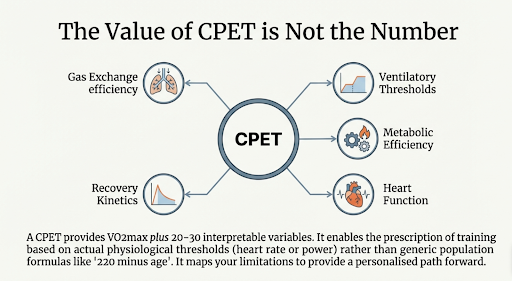
On the performance and optimisation front, it also lets you prescribe training from actual physiological heart rate or power thresholds rather than population-based formulas and estimates eg % of heart rate max.
That matters if you care about personalised and efficient progression in your training. Your targets are adapted to your physiology, not the population average.
So which is more useful: METs or VO2max?
It depends on the decision.
For public and population health
Estimated MET capacity is practical and scalable. It allows large health systems to stratify risk and track trends. It performs well because random individual error washes out in large samples.
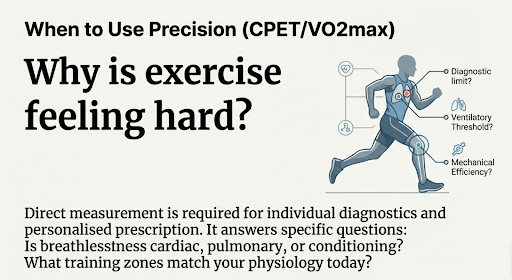
For an individual who wants personalised decisions
Direct measurement becomes more valuable when you need to answer specific questions:
Why does exercise feel disproportionately hard?
Is breathlessness cardiac, pulmonary, or conditioning?
What training zones match your physiology today?
Practical takeaways
Stop treating METs and VO2max as competing constructs. They are different ways of expressing the same underlying capacity, with very different measurement error.
Use estimated MET capacity when you want a cheap, rough risk stratification or a fitness ranking.
Use CPET when you need precision, explanation, or personalised prescription.
If you track VO2 estimates from a watch, focus on multi month direction, not weekly variation. The individual level error is not insignificant.
If you want one clean question to guide measurement choice: “Am I trying to predict risk, or am I trying to understand limitations and prescribe training?”
FAQs
Can CPET results be reported in METs?
Yes.
If VO2 is measured, METs are a unit conversion.
VO2 (mL per kg per minute) divided by 3.5 gives METs.
If most longevity studies use METs, should I ignore VO2peak?
No.
Outcome studies often rely on estimates because they scale.
That does not make direct measurement pointless.
Direct measurement becomes more valuable when you need individual level accuracy or diagnostic insight.
What is the simplest way to think about the difference?
CRF is the attribute.
VO2peak is a direct measurement of oxygen uptake at peak effort.
METs are a unit that can express measured oxygen uptake, or estimated oxygen uptake.
Further reading
[1] R. Ross et al., ‘Importance of Assessing Cardiorespiratory Fitness in Clinical Practice: A Case for Fitness as a Clinical Vital Sign’, Circulation, vol. 134, no. 24, pp. e653–e699, Dec. 2016, doi: 10.1161/CIR.0000000000000461.
[2] J. J. Lang et al., ‘Cardiorespiratory fitness is a strong and consistent predictor of morbidity and mortality among adults: an overview of meta-analyses representing over 20.9 million observations from 199 unique cohort studies’, May 2024, doi: 10.1136/bjsports-2023-107849.
[3] B. Singh et al., ‘Comparison of objectively measured and estimated cardiorespiratory fitness to predict all-cause and cardiovascular disease mortality in adults: A systematic review and meta-analysis of 42 studies representing 35 cohorts and 3.8 million observations’, J. Sport Health Sci., vol. 14, p. 100986, Dec. 2025, doi: 10.1016/j.jshs.2024.100986.
[4] ‘Association of muscle strength and cardiorespiratory fitness with all-cause and cancer-specific mortality in patients diagnosed with cancer: a systematic review with meta-analysis | British Journal of Sports Medicine’. Accessed: Feb. 25, 2026. [Online]. Available: https://bjsm.bmj.com/content/59/10/722.long
[5] ‘Cardiorespiratory fitness and cognitive function in middle age | Neurology’. Accessed: Feb. 25, 2026. [Online]. Available: https://www.neurology.org/doi/10.1212/WNL.0000000000000310?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed
[6] S. Wang et al., ‘Association of cardiorespiratory fitness with dementia risk across different levels of genetic predisposition: a large community-based longitudinal study’, Br. J. Sports Med., vol. 59, no. 3, pp. 150–158, Feb. 2025, doi: 10.1136/bjsports-2023-108048.
[7] ‘Metabolic Equivalent in Adolescents, Active Adults and Pregnant Women’. Accessed: Feb. 25, 2026. [Online]. Available: http://ouci.dntb.gov.ua/en/works/7XPgOB07/?utm_source=chatgpt.com
[8] K. Mandsager, S. Harb, P. Cremer, D. Phelan, S. E. Nissen, and W. Jaber, ‘Association of Cardiorespiratory Fitness With Long-term Mortality Among Adults Undergoing Exercise Treadmill Testing’, JAMA Netw. Open, vol. 1, no. 6, p. e183605, Oct. 2018, doi: 10.1001/jamanetworkopen.2018.3605.
[9] P. Kokkinos et al., ‘Cardiorespiratory Fitness and Mortality Risk Across the Spectra of Age, Race, and Sex’, J. Am. Coll. Cardiol., vol. 80, no. 6, pp. 598–609, Aug. 2022, doi: 10.1016/j.jacc.2022.05.031.
[10] S. Kodama et al., ‘Cardiorespiratory Fitness as a Quantitative Predictor of All-Cause Mortality and Cardiovascular Events in Healthy Men and Women: A Meta-analysis’, JAMA, vol. 301, no. 19, pp. 2024–2035, May 2009, doi: 10.1001/jama.2009.681.