
Why “normal” testosterone does not always mean normal function

Why is it that testosterone looks normal but you still have symptoms consistent with low testosterone?
Low libido.
Reduced energy.
Blunted drive.
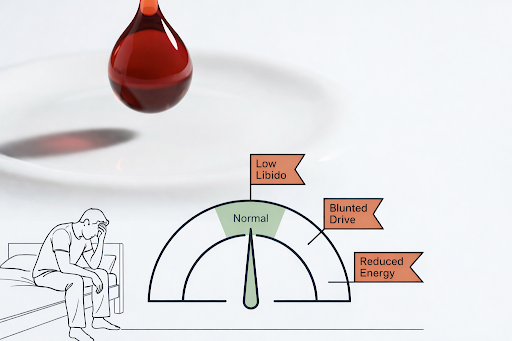
It is tempting to conclude: Testosterone is not the problem.
That is a conclusion too easy to arrive at.
This is one of the mismatches we often see in clinic, and it is not peculiar to testosterone.
Someone can be within the lab’s normal reference range, sometimes comfortably inside it, and still describe symptoms that are discordant with what the results are saying.
The evidence does not support diagnosing testosterone deficiency from symptoms alone. But it also does not support asserting that a normal total testosterone is the end of the conversation either.
Current guidelines require symptoms plus unequivocally low testosterone for diagnosis, while the physiology tells us that total testosterone is only one part of a wider system.
Furthermore, there is no consensus amongst specialist bodies as to what the lower threshold of total testosterone or free testosterone below which individuals will notice symptomatic improvements [1], [2], [3], [4].
The limitation of “normal range”
Reference ranges are statistical.
They tell you where a result sits relative to a reference population.
They do not tell you whether that value explains the person sitting in front of you or where that value lies in relation to their baseline.
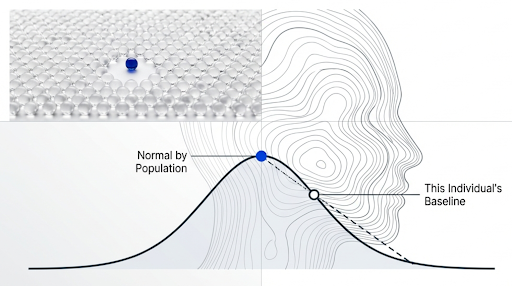
That distinction is important when we shift from a population medicine mindset, where decisions are orientated to what will work for most people, to what might be an approach that is most effective for the individual sitting in front of you.
Guidelines are clear that testosterone deficiency should be diagnosed only when symptoms coexist with unequivocally and consistently low serum testosterone. So a result inside the normal range tells you that the number is not overtly low by population standards. It does not tell you that testosterone function is normal in every practical sense, or that the symptoms must be coming from somewhere else.
In the absence of decent longitudinal data, it also does not inform us what the trajectory of those biomarkers looks like.
Total testosterone is only part of the signal
Many standard panels give you total testosterone.
But that is not the same as the biologically active levels.
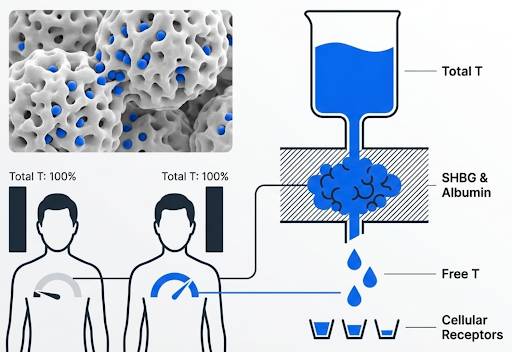
Testosterone circulates in our bodies in three broad fractions:
Bound tightly to SHBG.
Bound more loosely to albumin.
Free.
Only the free and loosely bound fractions are readily available at a tissue level. So two men can present with the same total testosterone levels and meaningfully different free testosterone because SHBG and albumin levels differ. SHBG and albumin level changes bioavailability, and bioavailability changes testosterone function [5].
Normal total testosterone does not exclude clinically relevant differences in how testosterone is actually available and working in the body.
Not necessarily deficiency. But not necessarily normal function either.
Symptoms are not driven by testosterone alone
Even when free testosterone is adequate, symptoms can persist.
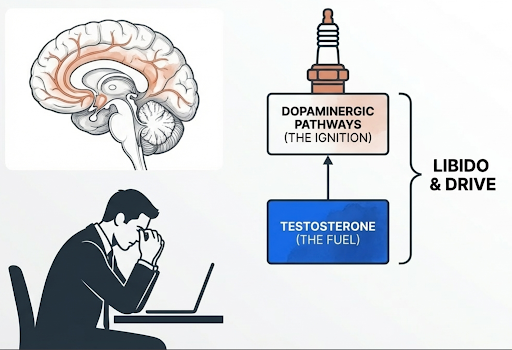
Testosterone contributes to libido, energy, mood, muscle maintenance, and recovery. But these are not purely dependent on testosterone levels. Libido and drive also depend on central neural systems, especially dopaminergic pathways and reward circuitry in the brain [6], [7], [8].
So even if a blood test shows testosterone is normal, problems in the brain systems that control desire, motivation, and reward can still be part of why someone has low libido or feels less driven.
Crucially, this is also where many people make assumptions, but normal testosterone does not prove the symptoms are unrelated to the hormonal axis.
But nor does it prove that testosterone treatment is the answer.
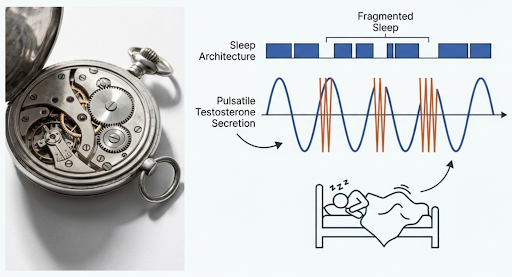
Sleep is a key regulator
One of the most consistently underestimated determinants of a well functioning hormonal axis is sleep.
Testosterone secretion is pulsatile and strongly influenced by sleep timing and sleep architecture, as we see with many hormone systems, such as cortisol and blood sugar control.
Controlled sleep restriction studies show lower daytime testosterone after short sleep in some research, and broader reviews support sleep as an important regulator of testosterone physiology [9], [10], [11].
The literature is not perfectly uniform. Not every study shows the same effect size, and not every protocol finds the same direction with the same magnitude [12]. But the overall strength of the research is credible enough to treat sleep as a first-order intervention rather than a nice-to-have.
This is important, because trying to interpret testosterone in isolation, while, for example, running on restricted or fragmented sleep, leads to an incomplete conclusion.
Why timing matters
Sleep disruption does not just influence testosterone quantity.
It can alter the timing of our natural hormone pattern. Sleep does not regulate testosterone in isolation. It also helps organise the wider endocrine environment in which testosterone is produced and functions.
Cortisol is part of that system. When sleep is restricted or fragmented, cortisol rhythm can become misaligned.
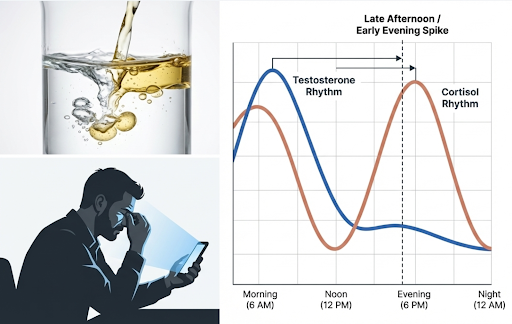
In controlled studies, substantial sleep restriction has been associated with higher late afternoon and early evening cortisol, suggesting that sleep loss can alter cortisol timing rather than simply raise total daily cortisol [13], [14], [15].
The point is not that cortisol is always grossly elevated. The point is that the rhythm can become misaligned. That altered hormonal context may affect recovery, energy, and the broader conditions in which testosterone signalling operates.
This is a whole-systems issue. Not just a single-biomarker problem.
Stress and central regulation
People in high-performance, demanding environments often live in sustained cognitive load.
That has consequences on the hormone axis.
Stress, including overtraining, can disrupt cortisol rhythms and can also reduce the strength of the brain signals involved in testosterone regulation, the hypothalamic-pituitary-gonadal axis [16]. It can also affect central drive. Libido and motivation are shaped by the brain circuits involved in reward, interest, and behaviour, not by testosterone alone. So symptoms such as low desire or reduced motivation may relate as much to brain regulation as to the testosterone level seen on a blood test.
This is one reason I would be cautious with a simplistic narrative such as testosterone is normal, so the symptoms cannot be hormonal.
That claim is wrong because it assumes the hormonal system begins and ends with a total testosterone value in isolation.
It does not.
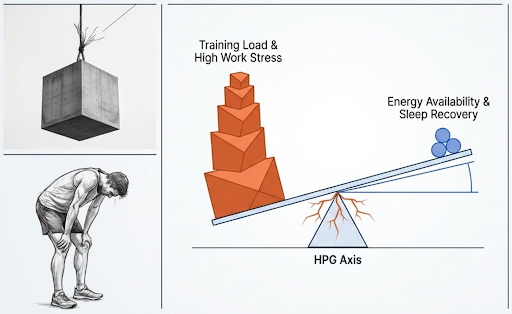
Training load and energy availability
In physically active men, another consideration presents itself.
High training loads combined with insufficient recovery or low energy availability can be associated with lower testosterone and altered hormonal pathways [16], [17].
This is well described in exercising males and endurance populations in the research. It does not require extreme overtraining or a dramatic collapse in performance.Early changes may be subtle and can include reduced libido, lower mood, impaired recovery, and stagnation or deterioration in performance or adaptation.
To put that in perspective, you can have someone who looks healthy on paper:
Good body composition.
Strong training consistency.
Reasonable total testosterone.
But still be experiencing:
Poor sleep.
High work stress.
Low recovery capacity.
Insufficient energy availability.
That is exactly the sort of person in whom the number can mislead you.
Why TRT is not always the answer
Testosterone replacement therapy has a clear place.
Conventional guidelines support its use when symptoms are present and testosterone is unequivocally and consistently low.
Outside that context, the narrative is less strong.
If testosterone is already within range, the chance that symptoms are being driven mainly by insufficient testosterone is less certain.
That means response to TRT is less predictable. Some men may report benefits. Others will not. The key point is that “symptoms plus a normal total testosterone” is not the same thing as a clean indication for treatment.
That is where the subtlety comes into the conversation.
The wrong conclusion is not only “TRT fixes this”.
The opposite conclusion is also wrong:
Normal testosterone means there is nothing to treat.
It means you need a better model.
A more useful way to think about it
Instead of asking:
Is testosterone normal?
I think the better question is:
Is testosterone function and central brain regulation aligned with the symptoms?
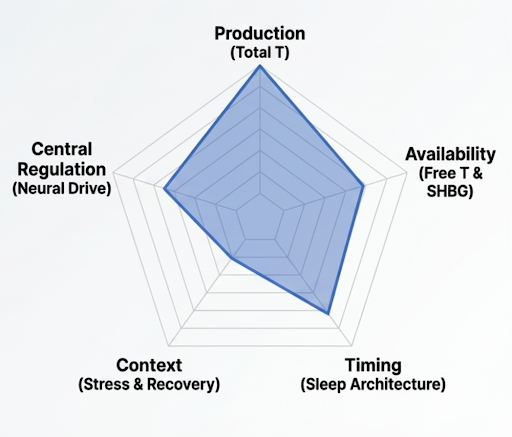
That pushes you to look at five domains, not one.
Production. Total testosterone.
Availability. SHBG and free testosterone.
Timing. Sleep-linked secretion and broader rhythm.
Central regulation. Hypothalamic signalling, dopaminergic tone, and drive.
Context. Stress, recovery, and energy availability.
This is much broader than a single lab result.
But it is closer to the reality.
Some people will still reasonably ask:
“More muscle mass is linked to better health and lower mortality. If testosterone can help me build more muscle, why would I not try it?”
It is a fair question.
But it mixes up three different things:
muscle mass as a marker of health
testosterone as a way to increase muscle
testosterone as a medical treatment
Those are not the same.
Lower lean mass is associated with higher mortality in observational studies, particularly in older and clinical populations [18], [19]. But that does not prove that raising muscle mass with testosterone in someone whose testosterone is already normal will improve long term health or reduce mortality. Association is not the same as proof of benefit from a drug intervention.
It is also true that testosterone can increase lean mass and strength even in healthy men who are not hypogonadal.
In a classic randomised trial, supraphysiological (higher levels than found naturally) testosterone increased fat-free mass, muscle size, and strength in normal men [20]. Dose-response work also showed that higher testosterone exposure produces greater anabolic effects [21]. So the muscle effect is real. But an anabolic effect is not the same as a medical indication, and it is not the same as proven long term health benefit.
If someone is truly hypogonadal, testosterone may be replacing something the body is not producing adequately.
If someone has normal testosterone, they are not correcting a clear deficiency. They are using a hormone to push physiology in a more anabolic direction.
Current guidelines support testosterone therapy when symptoms are present and testosterone is unequivocally and consistently low. They do not support it as a general muscle-optimisation strategy in eugonadal men.
That distinction is important because testosterone is not a benign intervention.
Once exogenous (additional) testosterone is started, the brain reduces key hormone (LH and FSH) signalling. That reduces the signals that tell your testes to make testosterone naturally. Your own production can fall, and sperm production can fall too. That matters for fertility, and it is one reason stopping can be difficult. Some men feel worse when they come off because their natural system takes time to recover [22].
Recovery after stopping is often possible, but it may take months and can take longer in some men, especially after more prolonged use.
There are other trade-offs as well. Testosterone can thicken the blood by increasing red blood cell levels, which is one of the common reasons treatment needs monitoring or dose adjustment [23]. It can worsen acne, contribute to breast tissue enlargement in some men, and may aggravate urinary symptoms in men with prostate enlargement. It also needs prostate monitoring in the right clinical context, because PSA and prostate-related follow-up become part of treatment.
Sleep is relevant too. Testosterone therapy is generally avoided or used cautiously in men with untreated severe obstructive sleep apnoea, because there is concern that it can worsen the condition in some cases.
So the key question is not:
“Can testosterone help build muscle?”
It can.
The better question is:
“If my testosterone is already normal, is using it to gain muscle a well-supported and low-risk way to improve long term health?”
At present, the evidence does not support a confident yes. The effect on muscle is established. The case for long term health benefit in men with normal testosterone is not.
What this changes in practice
If the symptoms and the numbers do not match, I would widen the frame before making a treatment decision.
I would look at:
Total testosterone, but not stop there.
SHBG and free testosterone.
Sleep duration, sleep regularity, and sleep quality.
Psychological stress and allostatic load.
Training load versus recovery.
Energy availability, especially in active men.
Treat total testosterone as one input, not the whole story.
Key Takeaways
Total testosterone does not fully testosterone exposure because SHBG changes bioavailability.
Sleep is an important regulator of testosterone physiology.
Central neural systems contribute to libido and drive.
Heavy training with low energy availability can be associated with lower testosterone and altered HPG-axis function.
Diagnosis of testosterone deficiency requires symptoms plus unequivocally low testosterone, not symptoms alone.
The evidence does not justify treating every symptomatic man with a normal total testosterone as a case for testosterone deficiency.
Bottom line
“Normal” testosterone does not guarantee normal function.
In some men, persistent symptoms may reflect altered bioavailability, disrupted sleep physiology, stress-related central effects, or an energy and recovery imbalance rather than testosterone deficiency.
Testosterone is part of a bigger, holistic systems picture. It is rarely the whole explanation.
The most useful approach is not to ignore the number, but not to treat it in isolation either. Treat it as one piece of a wider picture.
FAQs
1. Can you have low testosterone symptoms with normal testosterone?
Yes. You can have symptoms such as low libido, reduced energy, blunted drive, or poorer recovery even when total testosterone sits within the lab reference range. A normal result does not always mean testosterone is working normally at tissue level, and it does not rule out issues with free testosterone, SHBG, sleep, stress, or central brain regulation.
2. Why do I feel low testosterone symptoms if my blood test is normal?
Because total testosterone is only one part of the picture. Two people can have the same total testosterone but different free testosterone and different symptom patterns. Sleep disruption, stress, low energy availability, overtraining, and changes in brain reward and motivation pathways can all contribute to symptoms that look like low testosterone.
3. Does normal total testosterone mean testosterone is not the problem?
No. It means testosterone is not overtly low by population standards. It does not prove that testosterone function is normal in every practical sense, and it does not prove the symptoms are unrelated to the hormonal axis. It also does not automatically mean testosterone treatment is the right answer.
4. What is the difference between total testosterone and free testosterone?
Total testosterone is the full amount measured in the blood. Free testosterone is the small fraction not tightly bound to proteins and is more readily available to tissues. SHBG and albumin influence how much testosterone is actually bioavailable, which is why total testosterone alone can sometimes miss clinically relevant differences.
5. Can poor sleep lower testosterone or affect testosterone function?
Yes. Sleep is one of the most important regulators of testosterone physiology. Short, fragmented, or poor-quality sleep can lower testosterone in some studies and can also disrupt the wider hormone environment, including cortisol timing. This can affect energy, recovery, libido, and drive even if testosterone is not frankly low.
6. Can stress cause low libido or low drive even if testosterone is normal?
Yes. Libido and motivation are not driven by testosterone alone. They also depend on brain systems involved in reward, motivation, and behavioural drive. Chronic stress can disrupt cortisol rhythms and the brain signals involved in testosterone regulation, which may contribute to low desire, reduced motivation, and poorer recovery.
7. Can exercise or overtraining affect testosterone?
Yes. High training loads combined with poor recovery or low energy availability can be associated with lower testosterone and altered hormonal pathways. This is well described in physically active men and endurance populations. Early signs may include lower libido, lower mood, impaired recovery, and stalled adaptation rather than a dramatic collapse in performance.
8. Should I try TRT if I have symptoms but normal testosterone?
Not automatically. Conventional guidelines support testosterone replacement therapy when symptoms are present and testosterone is unequivocally and consistently low. If testosterone is already within range, the cause of symptoms is less clear, and response to TRT is less predictable. Symptoms plus normal testosterone is not the same as a clean indication for treatment.
9. If testosterone can increase muscle mass, why not use it for optimisation?
Because building muscle and treating deficiency are not the same thing. Testosterone can increase lean mass and strength, even in men without hypogonadism, but that does not prove it improves long-term health in men with normal testosterone. It is also not benign. It can suppress natural testosterone production, reduce sperm production, increase red blood cell levels, and create a monitoring burden.
10. What should be checked if symptoms and testosterone results do not match?
A broader assessment is usually more useful than repeating total testosterone alone. That may include free testosterone, SHBG, sleep duration and quality, stress load, training versus recovery, energy availability, and the wider clinical context. The more useful question is not simply whether testosterone is normal, but whether testosterone function and central regulation are aligned with the symptoms.
Further Reading
[1] B. Lunenfeld et al., ‘Recommendations on the diagnosis, treatment and monitoring of hypogonadism in men’, Aging Male, vol. 18, no. 1, pp. 5–15, Mar. 2015, doi: 10.3109/13685538.2015.1004049.
[2] S. Bhasin et al., ‘Testosterone Therapy in Men With Hypogonadism: An Endocrine Society Clinical Practice Guideline’, J. Clin. Endocrinol. Metab., vol. 103, no. 5, pp. 1715–1744, May 2018, doi: 10.1210/jc.2018-00229.
[3] J. P. Mulhall et al., ‘Evaluation and Management of Testosterone Deficiency: AUA Guideline’, J. Urol., vol. 200, no. 2, pp. 423–432, Aug. 2018, doi: 10.1016/j.juro.2018.03.115.
[4] G. Hackett et al., ‘The British Society for Sexual Medicine Guidelines on Male Adult Testosterone Deficiency, with Statements for Practice’, World J. Mens Health, vol. 41, no. 3, pp. 508–537, Jul. 2023, doi: 10.5534/wjmh.221027.
[5] N. Narinx et al., ‘Role of sex hormone-binding globulin in the free hormone hypothesis and the relevance of free testosterone in androgen physiology’, Cell. Mol. Life Sci. CMLS, vol. 79, no. 11, p. 543, Oct. 2022, doi: 10.1007/s00018-022-04562-1.
[6] R. S. Calabrò et al., ‘Neuroanatomy and function of human sexual behavior: A neglected or unknown issue?’, Brain Behav., vol. 9, no. 12, p. e01389, Sep. 2019, doi: 10.1002/brb3.1389.
[7] K. J. Jennings and L. de Lecea, ‘Neural and Hormonal Control of Sexual Behavior’, Endocrinology, vol. 161, no. 10, p. bqaa150, Aug. 2020, doi: 10.1210/endocr/bqaa150.
[8] M. R. Melis, F. Sanna, and A. Argiolas, ‘Dopamine, Erectile Function and Male Sexual Behavior from the Past to the Present: A Review’, Brain Sci., vol. 12, no. 7, p. 826, Jun. 2022, doi: 10.3390/brainsci12070826.
[9] R. Leproult and E. Van Cauter, ‘Effect of 1 Week of Sleep Restriction on Testosterone Levels in Young Healthy MenFREE’, JAMA, vol. 305, no. 21, pp. 2173–2174, Jun. 2011, doi: 10.1001/jama.2011.710.
[10] L. Su, S. Zhang, J. Zhu, J. Wu, and Y. Jiao, ‘Effect of partial and total sleep deprivation on serum testosterone in healthy males: a systematic review and meta-analysis’, Sleep Med., vol. 88, pp. 267–273, Dec. 2021, doi: 10.1016/j.sleep.2021.10.031.
[11] P. Y. Liu and R. T. Reddy, ‘Sleep, testosterone and cortisol balance, and ageing men’, Rev. Endocr. Metab. Disord., vol. 23, no. 6, pp. 1323–1339, 2022, doi: 10.1007/s11154-022-09755-4.
[12] I. Smith, I. Salazar, A. RoyChoudhury, and M.-P. St-Onge, ‘Sleep restriction and testosterone concentrations in young healthy males: Randomized controlled studies of acute and chronic short sleep’, Sleep Health, vol. 5, no. 6, pp. 580–586, Dec. 2019, doi: 10.1016/j.sleh.2019.07.003.
[13] R. Leproult, G. Copinschi, O. Buxton, and E. Van Cauter, ‘Sleep loss results in an elevation of cortisol levels the next evening’, Sleep, vol. 20, no. 10, pp. 865–870, Oct. 1997.
[14] K. Spiegel, R. Leproult, and E. Van Cauter, ‘Impact of sleep debt on metabolic and endocrine function’, Lancet, vol. 354, no. 9188, pp. 1435–1439, Oct. 1999, doi: 10.1016/S0140-6736(99)01376-8.
[15] N. A. O’Byrne, F. Yuen, W. Z. Butt, and P. Y. Liu, ‘Sleep and Circadian Regulation of Cortisol: A Short Review’, Curr. Opin. Endocr. Metab. Res., vol. 18, pp. 178–186, Jun. 2021, doi: 10.1016/j.coemr.2021.03.011.
[16] A. C. Hackney, ‘Hypogonadism in Exercising Males: Dysfunction or Adaptive-Regulatory Adjustment?’, Front. Endocrinol., vol. 11, p. 11, Jan. 2020, doi: 10.3389/fendo.2020.00011.
[17] M. Cupka and M. Sedliak, ‘Hungry runners – low energy availability in male endurance athletes and its impact on performance and testosterone: mini-review’, Eur. J. Transl. Myol., vol. 33, no. 2, p. 11104, Apr. 2023, doi: 10.4081/ejtm.2023.11104.
[18] G. Koon-Yee Lee et al., ‘Sarcopenia and mortality in different clinical conditions: A meta-analysis’, Osteoporos. Sarcopenia, vol. 7, no. Suppl 1, pp. S19–S27, Mar. 2021, doi: 10.1016/j.afos.2021.02.001.
[19] H.-H. Zhou, Y. Liao, Z. Peng, F. Liu, Q. Wang, and W. Yang, ‘Association of muscle wasting with mortality risk among adults: A systematic review and meta-analysis of prospective studies’, J. Cachexia Sarcopenia Muscle, vol. 14, no. 4, pp. 1596–1612, 2023, doi: 10.1002/jcsm.13263.
[20] S. Bhasin et al., ‘The effects of supraphysiologic doses of testosterone on muscle size and strength in normal men’, N. Engl. J. Med., vol. 335, no. 1, pp. 1–7, Jul. 1996, doi: 10.1056/NEJM199607043350101.
[21] S. Bhasin et al., ‘Testosterone dose-response relationships in healthy young men’, Am. J. Physiol. Endocrinol. Metab., vol. 281, no. 6, pp. E1172-1181, Dec. 2001, doi: 10.1152/ajpendo.2001.281.6.E1172.
[22] J. A. McBride and R. M. Coward, ‘Recovery of spermatogenesis following testosterone replacement therapy or anabolic-androgenic steroid use’, Asian J. Androl., vol. 18, no. 3, pp. 373–380, 2016, doi: 10.4103/1008-682X.173938.
[23] ‘The Effect of Route of Testosterone on Changes in Hematocrit: A Systematic Review and Bayesian Network Meta-Analysis of Randomized Trials | Journal of Urology’, J. Urol., Oct. 2021, Accessed: Mar. 29, 2026. [Online]. Available: https://www.auajournals.org/doi/10.1097/JU.0000000000002188