
The Physiology of Breath: Separating the clinical mechanics of nasal breathing from the wellness narrative
Breathwork has become mainstream wellness. The case for it is now firmly established in bestselling books, viral sleep hacks, and a steady stream of people asking about mouth taping, BOLT scores, and CO2 tolerance training. If you're genuinely curious about whether the air we move through our face via one route or another is something we should be optimising, read on.
Some of the more popular claims are based in solid physiological reality. Others are not. The two are not currently well distinguished in the wellness conversations.
The popular case for breath retraining
In its most favourable form, the popular thesis sounds like this. Modern humans breathe too much. Sedentary lives, anxiety, and processed food have produced a population that habitually over-breathes, lowering arterial CO2 and pushing the body into a chronic low-grade respiratory alkalosis (a mild shift in blood pH toward the non-acidic end, driven by CO2 being blown off faster than it is produced, due to the increased respiratory rate). This is said to make it harder for the blood to release oxygen into the tissues (the Bohr effect: haemoglobin grips oxygen more tightly when blood CO2 is low), shift the autonomic nervous system toward sympathetic dominance, and contribute to anxiety, fatigue, asthma symptoms and poor sleep.
The fix: to relearn how to breathe. Train CO2 tolerance through breath-holds. Track progress with a simple bedside measure called the BOLT score (the Body Oxygen Level Test, which is the number of seconds a person can comfortably hold their breath after a normal exhalation, without forcing air hunger). Move the air through the nose, not the mouth. Tape the mouth at night to keep the airway in the right mode. Periodically use deliberate cyclical hyperventilation, then breath-hold, to stress the system and build resilience.
This narrative has internal coherence. It draws on real physiology (the Bohr effect, autonomic effects of CO2, nitric oxide in the sinuses, the mechanical advantages of nasal resistance) and presents a single unifying lever (breath retraining) that promises to act on multiple problems at once. That is why it has gone mainstream.
Where the logic fails: the evidence skipped
The chronic over-breathing assertion doesn't tally with the data.
The pivotal trial is Hornsveld and colleagues 1996, a double-blind placebo-controlled study of the hyperventilation provocation test in 115 patients with suspected episodic or chronic hyperventilation syndrome [1]. The patients underwent a standard provocation (voluntary hyperventilation for several minutes) and a placebo experiment using isocapnic overbreathing, with carbon dioxide levels maintained by manual titration (CO2 was added back into the inspired air in real time to keep blood CO2 at its resting baseline, separating the act of breathing fast from the drop in CO2 it would otherwise cause).
The standard provocation reproduced patients' symptoms, but so did the placebo isocapnic version. Around a quarter of suspected hyperventilation syndrome patients did show symptoms with low CO2 levels, so acute drops in CO2 can reproduce symptoms in some. What the trial highlighted was not that low CO2 has any physiological effect (it clearly does), but not that those patients suffer from a chronic CO2-driven syndrome. Most have normal resting CO2, and 24-hour CO2 monitoring in the same study showed that when these patients had real-world symptomatic episodes, the fall in CO2 levels usually followed rather than preceded the onset of their symptoms.
The diagnostic label has been largely abandoned since. The field has largely accepted that the provocation test is invalid and that the classical syndrome has been overcalled for decades.
The studies in individuals at altitude is the second weakness. Over 200 million people live with sustained low arterial CO2 (around 29 mmHg) at chronic altitude. The body fully adapts: the kidneys correct blood pH within a few days, and the breathing-control sensors in the brain reset to the lower CO2 level [2], [3]. They do not show the autonomic instability, physical symptom clusters or general ill-health that lowland chronic over-breathing is said to produce. This is the most physiologically extreme natural experiment available that challenges the proposed physiology behind these statements.
The BOLT score, presented as a measure of CO2 tolerance, does not measure CO2 tolerance. Courtney and Cohen 2008 tested the underlying assumption directly in 83 adults and found that breath-hold time did not predict resting end-tidal CO2 [4]. Brearley and colleagues 2024 tested it against athletic performance in 49 elite speedskaters and found no correlation with any anaerobic or aerobic metric [5]. Breath-hold time reflects chemoreceptor tolerance (how long you can suppress the urge to breathe - an urge that the body's CO2 sensors generate as CO2 rises), lung volume, motivation and psychology. It does not reflect arterial CO2 or athletic capacity.
Thus, that modern humans chronically over-breathe is overstated and has no real supporting evidence. Modern population respiratory rates sit in the textbook normal range. The figures that circulate in breathwork literature trace back to one mid-twentieth-century clinician's observations and have not been replicated.
All is not lost: What the nose actually does that the mouth cannot
Challenging the underlying physiological claims does not strip the nose of its real value. Some specific benefits really do hold up.
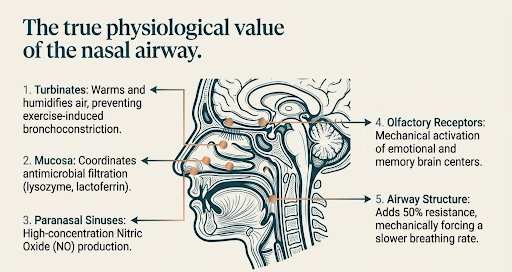
First, the nose conditions our inspired air. A large surface area of mucous membranes, turbulent flow over the turbinates, and a rich blood vessel network in our mucous membranes bring even cold dry air close to body temperature and full humidity by the time it reaches the throat.
Below a minute ventilation of around 35 L per minute (roughly the upper end of zone 2 cycling), the nasal route alone can keep up with demand for most adults. The original 1980 study found a mean switching point of 35.3 ± 10.8 L/min in two-thirds of healthy subjects (roughly 105 W of cycling), with the remainder splitting into habitual mouth-breathers and persistent nose-breathers [6]. Above that, the body switches to oronasal breathing. The practical implication is that most aerobic work below a lactate threshold zone is tolerable via nasal breathing.
Second, the nose protects against exercise-induced bronchoconstriction. Shturman-Ellstein and colleagues 1978 showed that nasal-only breathing produced near-complete inhibition of the post-exercise bronchoconstrictive response in asthmatic subjects, while mouth-only breathing exaggerated it [7]. The technical mechanism is that the nose warms and humidifies inhaled air, while the mouth delivers it cold and dry. Cold dry air reaching the lower airways dries out the thin fluid lining them, and that dehydration triggers the same inflammatory cascade that drives an asthma attack..
Third, the paranasal sinuses produce nitric oxide (NO) in high concentrations [8]. The NO produced in the sinuses is inhaled during nasal breathing and helps the lungs match airflow to blood flow, improving oxygen transfer to the blood. The effect is real and oral breathing bypasses it. One caveat worth naming: the popular extension of this finding into whole-body cardiovascular benefit is an overreach, because inhaled NO breaks down within seconds in the bloodstream, and systemic NO availability in humans is driven by dietary nitrate from food such as beetroot and leafy greens, not by sinus production.
Fourth, the act of breathing through the nose (rather than the mouth) drives synchronised electrical rhythms in the brain regions that handle emotion and memory. Zelano and colleagues 2016 demonstrated this directly using brain recordings from electrodes inside the skulls of epilepsy patients (already implanted for unrelated clinical reasons), with measurable behavioural effects: faster recognition of fearful faces and better memory recall during nasal but not oral breathing [9]. The mechanism is mechanical activation of smell-receptor cells in the upper nose. This is unique to the nasal route, not just to slower breathing.
Fifth, the nose filters incoming air. Turbulent flow over the turbinates traps particulates, and the nasal mucus carries a coordinated antimicrobial defence (lysozyme, lactoferrin, secretory IgA, and a continuous low level of nitric oxide). Oral breathing bypasses this filter entirely. The mechanistic argument for nasal filtration as a contributor to upper respiratory defence is strong but currently lacking in direct outcome evidence.
Why most "nasal breathing benefits" are really slow breathing benefits
Most popular accounts miss the message that actually reflects a story worth telling. The cardiovascular and autonomic benefits most often attributed to nasal breathing are largely benefits of the slow deep pattern that nasal resistance imposes, delivered via the nasal route.
Slow breathing at around six breaths per minute generates resonance between respiratory sinus arrhythmia and the body's blood-pressure feedback loop (the baroreflex). The pattern maximises heart rate variability (the beat-to-beat swing in heart rate that marks healthy autonomic balance), improves the baroreflex, lowers blood pressure, and has a calming effect on anxiety.
This rate also appears to be the physiological convergence point of several contemplative traditions: Bernardi, Sleight and colleagues 2001 showed that the Latin rosary recited at its traditional cadence and the yogic mantra "Om mani padme hum" both pace respiration to around six breaths per minute, with the same enhanced cardiovascular synchronisation seen with laboratory-paced slow breathing [10].
The wider evidence base for slow breathing is the strongest in breathing physiology. In patients with chronic heart failure and high blood pressure, slow breathing at around six breaths per minute sharpens the body's blood-pressure feedback loop and lowers blood pressure [11], [12]. Most of the modern clinical trial evidence is on a structured version of the same practice, called HRV biofeedback, where the person watches their heart rate variability on a screen and learns to maximise it by adjusting their breathing rhythm. A 2020 meta-analysis of 58 trials of HRV biofeedback found the largest improvements in anxiety, depression and performance outcomes [13].
The mechanism is the syncing of breath with the body's blood-pressure feedback loop at six breaths per minute, not a correction of some chronic CO2 deficit. The blood pressure and autonomic gains depend on the rhythm, not the route. They appear whether the slow pattern is achieved through the nose or through the mouth, as long as the rate matches.
Where does the nose then add value? Three places. It imposes the slow pattern through its resistance (around 50% of total airway resistance), so most people who set out to breathe nasally will end up breathing more slowly without consciously aiming for it. Second, only nasal airflow activates the brain-rhythm syncing in the emotional and memory centres described above. Third, it delivers the lung benefits of warming and moistening the inhaled air, and autoinhaling nitric oxide from the sinuses to help oxygen transfer. That is the complete cardiovascular and cognitive case for the nose. It is enough.
Putting this all together
Breathing retraining is a very reasonable, zero-cost intervention.
For increasing performance, the case for nasal breathing is for submaximal aerobic training, not for maximal effort. At zone 2 intensities (moderate aerobic effort at a conversational pace, which makes up the bulk of most people's training), nasal-only breathing produces slower, deeper breaths, more CO2 retained between breaths, and a lower total volume of air moved for the same workload. The result is a more efficient breathing pattern: around 9% more efficient in healthy adults and up to 35% more efficient in heart failure patients during submaximal cycling [14], [15].
Practically, this translates to lower perceived effort at the same workload, more sustainable easy-aerobic work, and exercise induced bronchospasm. What it does not deliver is an increased VO2max or peak power. Multiple studies have tested this directly. In adapted recreational runners and in well-trained endurance athletes, nasal-only breathing leaves VO2max and peak power unchanged [15], [16], [17].
For cognitive performance, nasal breathing synchronises rhythms in the brain's emotional and memory centres; oral breathing does not. The measurable behavioural effects from controlled studies are small acute effects, not large outcome trials. The mechanistic logic for breathing nasally during sustained focused work, or in the run-up to a high-stakes conversation, is reasonable. The outcome evidence is limited at this point in time.
In sleep-disordered breathing, the nose is the favoured route: forced oral breathing raises upper airway resistance approximately 2.5-fold and dramatically increases obstructive airways [18]. In asthma with co-existing dysfunctional breathing (around 29% of treated UK primary care asthmatics), physiotherapy-led breathing retraining improves asthma-specific quality of life without changing lung function or inhaler use [19], [20]. In panic specifically, breathing retraining matches but does not beat cognitive therapy [21]. The common thread across these clinical use cases is that it targets the symptomatic burden of co-existing abnormal breathing patterns, not the underlying disease.
There are a couple of safety consideration that are often left unaddressed.
Mouth taping in unscreened adults is not currently established as safe. The evidence base is a recent scoping review of nine small studies, with an early suggestion of possible benefit in mild obstructive sleep apnoea (OSA) mouth-breathers who have already had their nasal airway confirmed as being patent [22]. Safety in undiagnosed moderate-to-severe OSA, or in patients with fixed nasal obstruction, is not established.
Some popular breathing methods combine many rapid deep breaths in a row with breath-holds afterwards. In experiments where researchers deliberately triggered an inflammatory immune response in healthy volunteers (by injecting a small dose of bacterial endotoxin), trained practitioners of the technique showed a measurable reduction in that inflammation. The breathing component, not the cold exposure that often accompanies these methods, was driving the effect [23]. The clinical translation beyond endotoxin challenge is unproven.
The safety issue is concrete. Deliberate hyperventilation followed by breath-hold can cause loss of consciousness on its own, and the practice has caused multiple drownings when performed in or near water. The popular pairing with cold-water immersion adds a separate cardiac risk. Cold immersion activates the sympathetic nervous system while breath-hold activates the parasympathetic, and the simultaneous opposing drives (what cardiology calls "autonomic conflict") trigger cardiac arrhythmia in around 2% of healthy adults during free-breathing cold immersion, but in 62 to 82% when the immersion is preceded by breath-holding [24]. Even experienced Korean breath-hold divers show arrhythmia rates of 43% in summer and 72% in winter. Real-world deaths have followed practitioners performing the technique in pools, lakes and ice baths [25]. The practice should not be performed in or near water, and the cold-immersion-plus-hyperventilation combination should be avoided entirely in anyone with known or suspected cardiac risk.
Anyone with significant breathlessness, suspected dysfunctional breathing, asthma that feels poorly controlled, or possible OSA should be assessed by a clinician rather than relying on a wellness app or a book.
What can healthy individuals looking to improve their breathing actually do:
Default to nasal breathing through aerobic work below threshold. The switching point sits around 35L per minute minute ventilation (which was on average roughly 105 W of cycling), so most zone 2 work would tolerate nasal breathing. Nasal-only work does not improve maximal performance.
Try five minutes of slow nasal breathing at around six breaths per minute (a four-second inhale and a six-second exhale, or similar) before sleep, or before a high-stakes conversation. The mechanism is baroreflex resonance [26]. The effect on acute autonomic balance is the most replicated finding in the slow-breathing literature.
If symptomatic with asthma, panic, suspected dysfunctional breathing, or possible OSA, ask your doctor about a referral to a respiratory physiotherapist for formal Papworth-style breathing retraining (or a sleep clinic for OSA assessment) rather than starting a self-directed practice. Do not mouth-tape without an OSA screen. Do not perform deliberate hyperventilation near water.
Q&A
Q1. Don't we all chronically over-breathe? Isn't that what's wrong with modern life?
No. Peer-reviewed evidence does not show that the modern general population breathes faster, or with lower arterial CO2, than historical populations. The pivotal trial of the chronic-hyperventilation "syndrome" found that symptoms attributed to over-breathing were equally reproduced in a placebo isocapnic condition where CO2 was held normal. Over 200 million altitude residents live with sustained low CO2 and do not show the symptom complex attributed to lowland over-breathers.
Q2. If slow breathing is the real signal, does it matter whether I breathe through my nose?
Yes, but not for the cardiovascular reasons usually given. Most of the blood pressure and heart rate variability gains attributed to nasal breathing are slow-pattern effects, and will appear when the same rate is achieved orally. The route-specific benefit of the nose is in three other places: conditioning of inspired air (relevant for asthma and exercise-induced bronchoconstriction), local lung nitric oxide inhalation, and the brain effects (olfactory-limbic cortical entrainment) with measurable cognitive effects. And the nose imposes the slow pattern through its resistance, which is most of the practical reason to use it.
Q3. Should I mouth-tape at night?
Not routinely, and not without an OSA assessment first. The evidence base for nocturnal mouth taping is small and is concentrated in patients with mild OSA who have already had their nasal airway confirmed patent. Safety in undiagnosed moderate-to-severe OSA or with fixed nasal obstruction is not established. If a patient is snoring or sleeping badly, the right next step is a sleep clinic referral, not a strip of tape.
Q4. Is the BOLT score worth tracking?
Not as the popular case presents it. Breath-hold time does not predict resting arterial CO2 and does not correlate with athletic performance in elite athletes. It is a reasonable within-subject change marker during a structured breathing-retraining course where technique and motivation are held constant. As a between-person measure of CO2 tolerance, fitness or general health, it is not helpful.
Q5. Will nasal-only training improve my VO2max or peak power?
No. The randomised crossover and chronic-adaptation studies converge: nasal-only breathing does not improve maximal performance, and in unadapted subjects forcing the route at maximal effort will reduce achievable work. In adapted subjects, performance is preserved, not enhanced. At submaximal intensities, nasal breathing improves ventilatory efficiency and protects against exercise-induced bronchoconstriction. Use it as a tool for zone 2 work and asthma management, not as a top-end performance enhancer.
Further Reading
[1] H. K. Hornsveld, B. Garssen, M. F. Dop, P. van Spiegel, and J. de Haes, ‘Double-blind placebo-controlled study of the hyperventilation provocation test and the validity of the hyperventilation syndrome’, The Lancet, vol. 348, no. 9021, pp. 154–158, Jul. 1996, doi: 10.1016/S0140-6736(96)02024-7.
[2] R. Krapf, I. Beeler, D. Hertner, and H. N. Hulter, ‘Chronic Respiratory Alkalosis’, N. Engl. J. Med., vol. 324, no. 20, pp. 1394–1401, May 1991, doi: 10.1056/NEJM199105163242003.
[3] G. Zubieta-Calleja, G. Zubieta-Castillo, L. Zubieta-Calleja, G. Ardaya-Zubieta, and P.-E. Paulev, ‘Do Over 200 Million Healthy Altitude Residents Really Suffer from Chronic Acid–Base Disorders?’, Indian J. Clin. Biochem., vol. 26, no. 1, pp. 62–65, Jan. 2011, doi: 10.1007/s12291-010-0088-9.
[4] R. Courtney and M. Cohen, ‘Investigating the Claims of Konstantin Buteyko, M.D., Ph.D.: The Relationship of Breath Holding Time to End Tidal CO2 and Other Proposed Measures of Dysfunctional Breathing’, J. Altern. Complement. Med., vol. 14, no. 2, pp. 115–123, Mar. 2008, doi: 10.1089/acm.2007.7204.
[5] T. Kowalski, K. Rebis, A. Wilk, A. Klusiewicz, S. Wiecha, and B. Paleczny, ‘Body Oxygen Level Test (BOLT) is not associated with exercise performance in highly-trained individuals’, Front. Physiol., vol. 15, Aug. 2024, doi: 10.3389/fphys.2024.1430837.
[6] V. Niinimaa, P. Cole, S. Mintz, and R. J. Shephard, ‘The switching point from nasal to oronasal breathing’, Respir. Physiol., vol. 42, no. 1, pp. 61–71, Oct. 1980, doi: 10.1016/0034-5687(80)90104-8.
[7] R. Shturman-Ellstein, R. J. Zeballos, J. M. Buckley, and J. F. Souhrada, ‘The beneficial effect of nasal breathing on exercise-induced bronchoconstriction’, Am. Rev. Respir. Dis., vol. 118, no. 1, pp. 65–73, Jul. 1978, doi: 10.1164/arrd.1978.118.1.65.
[8] J. O. N. Lundberg et al., ‘High nitric oxide production in human paranasal sinuses’, Nat. Med., vol. 1, no. 4, pp. 370–373, Apr. 1995, doi: 10.1038/nm0495-370.
[9] ‘Nasal Respiration Entrains Human Limbic Oscillations and Modulates Cognitive Function | Journal of Neuroscience’. Accessed: May 30, 2026. [Online]. Available: https://www.jneurosci.org/content/36/49/12448
[10] L. Bernardi et al., ‘Effect of rosary prayer and yoga mantras on autonomic cardiovascular rhythms: comparative study’, BMJ, vol. 323, no. 7327, pp. 1446–1449, Dec. 2001, doi: 10.1136/bmj.323.7327.1446.
[11] L. Bernardi et al., ‘Slow Breathing Increases Arterial Baroreflex Sensitivity in Patients With Chronic Heart Failure’, Circulation, vol. 105, no. 2, pp. 143–145, Jan. 2002, doi: 10.1161/hc0202.103311.
[12] C. N. Joseph et al., ‘Slow Breathing Improves Arterial Baroreflex Sensitivity and Decreases Blood Pressure in Essential Hypertension’, Hypertension, vol. 46, no. 4, pp. 714–718, Oct. 2005, doi: 10.1161/01.HYP.0000179581.68566.7d.
[13] P. Lehrer et al., ‘Heart Rate Variability Biofeedback Improves Emotional and Physical Health and Performance: A Systematic Review and Meta Analysis’, Appl. Psychophysiol. Biofeedback, vol. 45, no. 3, pp. 109–129, Sep. 2020, doi: 10.1007/s10484-020-09466-z.
[14] P. Eser et al., ‘Improved exercise ventilatory efficiency with nasal compared to oral breathing in cardiac patients’, Front. Physiol., vol. 15, Aug. 2024, doi: 10.3389/fphys.2024.1380562.
[15] G. M. Dallam, S. R. McClaran, D. G. Cox, and C. P. Foust, ‘Effect of Nasal Versus Oral Breathing on Vo2max and Physiological Economy in Recreational Runners Following an Extended Period Spent Using Nasally Restricted Breathing’, Int. J. Kinesiol. Sports Sci., vol. 6, no. 2, pp. 22–29, Apr. 2018, doi: 10.7575/aiac.ijkss.v.6n.2p.22.
[16] J. Bergqvist et al., ‘Effects of oral, oronasal, and oronasal breathing with a decongested nose during incremental maximal exercise testing of well-trained endurance athletes: a randomized cross-over study’, Front. Physiol., vol. 16, Sep. 2025, doi: 10.3389/fphys.2025.1654725.
[17] M. Mapelli et al., ‘Nasal vs. oral BREATHing WIn Strategies in healthy individuals during cardiorespiratory Exercise testing (BreathWISE)’, PloS One, vol. 20, no. 7, p. e0326661, 2025, doi: 10.1371/journal.pone.0326661.
[18] M. F. Fitzpatrick, H. McLean, A. M. Urton, A. Tan, D. O’Donnell, and H. S. Driver, ‘Effect of nasal or oral breathing route on upper airway resistance during sleep’, Eur. Respir. J., vol. 22, no. 5, pp. 827–832, Nov. 2003, doi: 10.1183/09031936.03.00047903.
[19] M. Thomas, R. K. McKinley, E. Freeman, and C. Foy, ‘Prevalence of dysfunctional breathing in patients treated for asthma in primary care: cross sectional survey’, BMJ, vol. 322, no. 7294, pp. 1098–1100, May 2001, doi: 10.1136/bmj.322.7294.1098.
[20] A. Bruton et al., ‘Physiotherapy breathing retraining for asthma: a randomised controlled trial’, Lancet Respir. Med., vol. 6, no. 1, pp. 19–28, Jan. 2018, doi: 10.1016/S2213-2600(17)30474-5.
[21] A. E. Meuret, D. Rosenfield, A. Seidel, L. Bhaskara, and S. G. Hofmann, ‘Respiratory and cognitive mediators of treatment change in panic disorder: Evidence for intervention specificity’, J. Consult. Clin. Psychol., vol. 78, no. 5, pp. 691–704, 2010, doi: 10.1037/a0019552.
[22] S. K. Fangmeyer, C. D. Badger, and P. G. Thakkar, ‘Nocturnal mouth-taping and social media: A scoping review of the evidence’, Am. J. Otolaryngol., vol. 46, no. 1, p. 104545, Jan. 2025, doi: 10.1016/j.amjoto.2024.104545.
[23] M. Kox et al., ‘Voluntary activation of the sympathetic nervous system and attenuation of the innate immune response in humans’, Proc. Natl. Acad. Sci., vol. 111, no. 20, pp. 7379–7384, May 2014, doi: 10.1073/pnas.1322174111.
[24] M. J. Shattock and M. J. Tipton, ‘“Autonomic conflict”: a different way to die during cold water immersion?’, J. Physiol., vol. 590, no. 14, pp. 3219–3230, 2012, doi: 10.1113/jphysiol.2012.229864.
[25] K. T. and | K. Southern, ‘Wim Hof started a cold water therapy trend. Our daughters died trying it’. Accessed: May 30, 2026. [Online]. Available: https://www.thetimes.com/uk/society/article/wim-hof-iceman-breathing-method-cold-water-therapy-killed-9tnvc5w8q
[26] M. A. Russo, D. M. Santarelli, and D. O’Rourke, ‘The physiological effects of slow breathing in the healthy human’, Breathe, vol. 13, no. 4, pp. 298–309, Nov. 2017, doi: 10.1183/20734735.009817.