
When a "natural" supplement is not: red yeast rice and the four questions before you buy any supplement
A four-question test for any supplement, including the one you are considering right now.

The story most people missed
In 2024, more than 100 people in Japan developed a serious form of kidney injury that prevents the kidneys reabsorbing glucose, amino acids, and phosphate from the urine, a condition called Fanconi syndrome. At least 76 of them died. The product was beni-koji, a fermented rice supplement sold by Kobayashi Pharmaceutical for cholesterol support[1].
The story did not travel widely outside Japan. In the supplement aisles of London, New York, or Milan, very little visibly changed. The product family that contains beni-koji, rice fermented with moulds of the Monascus genus, is sold across most Western markets under different names and different specifications. The most common cousin is red yeast rice, marketed as a "natural" cholesterol-lowering supplement.
A reasonable person reading the headline would conclude that fermented rice supplements are dangerous, or that the Japanese product was contaminated. Each of those conclusions is partly right and mostly wrong. The deaths matter. So does what they reveal about how we evaluate any supplement.
The Japanese deaths are not the full picture but lean into a more important question.
The wrong question
When a patient asks about red yeast rice, the question they usually mean is something like: should I take a supplement instead of a statin? Or: is the natural option safer than the pharmaceutical option?
These are the wrong questions. They sound reasonable, but they result in bad decisions.
This is not an argument that supplements are categorically worse than pharmaceuticals. Some pharmaceuticals are dangerous. Some supplements are excellent. The categories themselves do not tell you what you need to know to make a good decision.
A better test, transferrable to any supplement rather than only this one, is four questions.
What is actually in the bottle, and how is it regulated? Active ingredient, dose, standardisation, contamination risk.
What does the evidence say about the outcome that really matters to you? Not what the marketing claims. Not what mechanism predicts. What clinical studies actually measured, and how confident we can be in the result.
What is the safety and interaction profile? Side effects, monitoring needs, interactions, contraindications, and crucially, what it does in combination with the other things in your life.
Does the studied population match yours? A drug or supplement is only "effective" or "safe" in the population it was studied in. The trial subjects might not be you.
Red yeast rice is a useful case to work through, because it has the most consistent evidence base of any cholesterol-lowering supplement, the most established mechanism of action, and the most underappreciated risk profile. If the four questions cannot give you a clear answer here, they will struggle to give you a clear answer anywhere.
What is actually in the bottle?
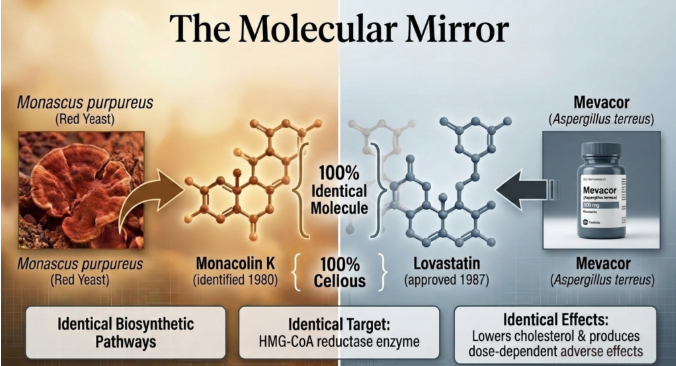
Red yeast rice is white rice fermented with the mould Monascus purpureus. The fermentation produces a family of compounds called monacolins. The most active of these is monacolin K.
Monacolin K is, molecule for molecule, lovastatin[2]. Lovastatin was the first statin to reach the market, approved by the FDA in 1987 as a prescription cholesterol-lowering drug. The supplement and the prescription drug are not chemical cousins. They are the very same compound, derived from the same biosynthetic pathway, hitting the same target in the liver, an enzyme called HMG-CoA reductase that controls the body's cholesterol production. They produce the same effects on cholesterol and the same adverse effects in proportion to dose.
This single point reframes every other way we think about red yeast rice. The supplement is a statin. The relevant comparison is not statin versus supplement; it is regulated statin versus unregulated statin.
The regulation matters because the monacolin K content of red yeast rice products varies enormously. In China, a standardised extract called Xuezhikang is licensed as a lipid-lowering drug and contains around 10 mg monacolin K daily at standard dose. In Europe, the European Food Safety Authority concluded in 2018 that no safe upper limit could be established for monacolin K from food supplements [3]. The European Commission subsequently restricted supplements containing 3 mg or more of monacolin K per daily dose, with most member states applying the cap from 2022 [4]. Many products that previously sold 10 mg-per-day formulations were reformulated below 3 mg, where the lipid effect becomes substantially smaller. In the United States, the FDA classifies high-monacolin red yeast rice products as unapproved drugs, though enforcement is inconsistent [5].
Independent laboratory analyses of red yeast rice products have repeatedly found monacolin K content varying by more than 100-fold across the recommended daily doses on the label, and some products with no detectable monacolin K at all [6]. A separate quality risk is contamination with citrinin, a kidney-damaging fungal toxin that Monascus moulds can produce under certain fermentation conditions.
This brings us back to beni-koji. The Japanese product associated with the 2024 deaths was made with a different mould, Monascus pilosus, not the Monascus purpureus that produces standard red yeast rice. The compound that caused the kidney injury has not yet been identified in published case series, but is thought to be an unknown by-product of the beni-koji fermentation rather than monacolin K itself [1]. The beni-koji kidney-injury signal does not transfer cleanly to standard Western red yeast rice products.
The principle it illustrates does transfer. Fermentation of any rice product with any fungus, at industrial scale, with weak regulatory oversight on the active and contaminant compounds, is a chemistry problem with potential significant health consequences. Beni-koji is the evidence for this and the assumption you make by taking them is that the bottle contains the dose on the label, made with the species on the label, free of contaminants the label does not mention.
What does the evidence actually say?
The evidence for cholesterol lowering is, by supplement standards, pretty consistent. The most recent meta-analyses converge on red yeast rice reducing LDL cholesterol by 25% to 35% versus placebo, equivalent to an absolute reduction of roughly 0.9 to 1.0 mmol/L in patients with mild-to-moderate dyslipidaemia [7]. The effect size is broadly equivalent to low-intensity prescription statin therapy, which is unsurprising given that the active ingredient is, again, a statin.
Triglyceride and HDL effects are smaller, less consistent, and the certainty is low.
The hard outcome data, whether red yeast rice reduces heart attacks, strokes, and deaths, rests almost entirely on a single trial. The China Coronary Secondary Prevention Study (CCSPS) randomised 4,870 patients in China who had previously had a heart attack to either Xuezhikang at 1,200 mg per day, providing approximately 10 mg of monacolin K, or placebo, and followed them for an average of 4.5 years [8]. The result was a 45% relative reduction in major cardiovascular events and a 33% reduction in all-cause mortality.
That is a striking number. It is also a single trial, in a Chinese population, conducted before modern background therapy was widespread. Very few of the participants were on a prescription statin, on a blood-pressure medicine of the ACE-inhibitor class, or on anti-clotting (antiplatelet) medication at baseline, because Chinese clinical practice in the late 1990s did not routinely use them. The trial was open-label. The product, Xuezhikang, is not widely available outside China. No independent trial has replicated the CCSPS magnitude of cardiovascular benefit in a modern Western population on background therapy.
The honest reading is that red yeast rice probably reduces cardiovascular events, by a magnitude consistent with what its LDL effect would predict, in patients who would otherwise be on nothing. Whether the same drug, in the same dose, adds anything meaningful on top of a modern lipid-lowering regimen is not known.
Who should not take this?
Because the active ingredient is lovastatin, the rules for taking it safely are the rules for taking a statin safely. There are three particularly clinically important interactions to know, but this highlights a reminder for anyone taking a supplement, you should always discuss this with your doctor, especially this one:
Other statins. If you are already taking a prescription statin, adding red yeast rice is taking two statins. The risk of muscle injury, and the rare severe form in which damaged muscle protein leaks into the bloodstream and can injure the kidneys (rhabdomyolysis), rises with dose. This is the easiest way to accidentally double the dose. It is the most common interaction patients miss, because they do not realise the supplement is the same drug class.
Macrolide antibiotics, particularly clarithromycin. Clarithromycin is one of the most commonly prescribed antibiotics for chest infections, sinusitis, and dental work. It is a potent blocker of the main liver enzyme that breaks down lovastatin (CYP3A4). Combining the two pushes statin blood levels up sharply and is a well-documented trigger for muscle injury [9]. The practical implication is that if your GP prescribes clarithromycin, pause the red yeast rice for the antibiotic course.
Significant grapefruit juice intake. Grapefruit contains compounds (furanocoumarins) that block the same drug-breakdown enzyme in the gut. The interaction is dose-dependent. A daily large glass of grapefruit juice can roughly double lovastatin exposure; sustained heavy intake can multiply it many-fold [10]. This is the interaction patients least expect, because a food and a supplement do not feel like a drug combination.
Beyond those three, there are more absolute contraindications worth knowing, and are listed in the Q&A at the end of this piece but are not comprehensive.
The clinical action that follows is also the same as for a statin. Baseline measurement of blood tests, including liver enzymes. Symptom check for new muscle pain, weakness, or dark urine, and about yellowing of the skin or eyes (jaundice) or pain in the upper-right side of the abdomen. A medication review at any new prescription. None of this is exotic. It is the standard of care for the drug class red yeast rice belongs to, whether the bottle says "supplement" or not and why you should always speak to your doctor before starting this supplement.
Real-world safety monitoring (pharmacovigilance) data, drawn from millions of consumer-years of monitored use, suggest the overall rate of reported adverse events is low, around 0.04% per consumer-year of use, with serious events one to two orders of magnitude lower [14]. That reads reassuringly until you remember that voluntary safety-monitoring systems under-report serious events by an order of magnitude, that most users are not being monitored at all, and that population averages do not protect the individual taking the interacting medication.
Does this map to a modern Western patient?
The patients in the CCSPS were Chinese, treated after a heart attack (a myocardial infarction), and largely untreated by modern standards. Most often, the individual looking to add red yeast rice to their supplement stack is usually different in three ways: they have not yet had a heart attack, are on or considering a modern lipid-lowering regimen, and are asking about red yeast rice because they want to avoid a statin.
That mismatch is the centre of the problem. A trial result is only "evidence for you" if your circumstances are close enough to the trial population that the same result is plausible. CCSPS-magnitude benefit is unlikely to transfer to a primary prevention patient at borderline risk, on no other therapy, in a modern Western context. The truthful answer is that we do not know what red yeast rice adds for that patient.
We can ask a better question. How strong is the case for lipid-lowering at all for a particular person? Population risk calculators that lump in age and crude lipid panels have well-known limits, and a tendency to delay action until risk has already accumulated. Lifetime risk calculators are getting better and more widely used now. A more precise approach reads cardiovascular risk from three pieces of information used together.
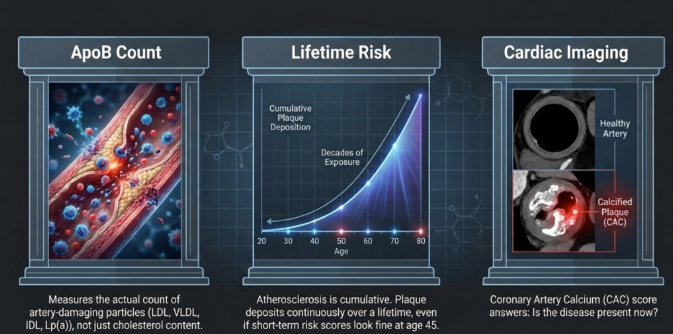
The total count of artery-damaging cholesterol particles in the blood (apoB). ApoB counts every particle in the bloodstream that physically embeds in artery walls, which includes LDL, VLDL, IDL, and lipoprotein(a). The standard cholesterol panel measures LDL-C, the cholesterol content of those particles, but the particle count is a stronger predictor of cardiovascular events. Two patients with the same LDL cholesterol can have very different particle counts, and the particle count is what does the damage [15]. For a longer treatment of apoB in cardiovascular risk and how I use it in practice, see Part 1 and Part 2.
Lifetime risk rather than ten-year risk, calculated from cumulative exposure to high apoB over decades. Plaque build-up in the arteries (atherosclerosis) is a slow, cumulative process. The person whose apoB has been sitting in the upper half of the reference range since their twenties is depositing plaque continuously, even if their ten-year risk score is reassuring at forty-five [16].
Cardiac imaging where indicated. The most common test is a CT scan that measures calcified plaque in the heart's arteries (the coronary artery calcium, or CAC, score). Other options are a neck-artery ultrasound that measures early thickening of the arterial wall (carotid intima-media thickness) or a CT scan of the heart arteries themselves (CT coronary angiography). Imaging answers a different question: not "what is your risk?" but "is the disease present now?" A zero CAC score in middle age genuinely lowers the urgency. A high CAC score raises it considerably regardless of what the calculator says.
Apply that framework to the red yeast rice question, and the four-question test gives a cleaner answer.
If your apoB is clearly elevated, your imaging shows established early plaque in the arteries before any symptoms, and your lifetime exposure has been high, the case for lipid-lowering is strong. In that situation, a quarter-dose unregulated statin in a capsule with variable monacolin K content is not a softer choice. It is the same drug class, less reliable in dose, with weaker monitoring, doing a smaller version of the job a prescription statin would do properly.
If your apoB is at the upper end of the population range, your imaging is clean, and your lifetime trajectory is rising but you are not yet in a high-risk band, the case for lipid-lowering is genuinely borderline. Lifestyle work, the things that move apoB at the metabolic level, mostly nutrition, body composition, and exercise pattern, take first place. If a pharmacological agent is added at that stage, the choice between red yeast rice and low-dose statin is mostly about regulatory reliability, monitoring, and your tolerance, not about one being meaningfully gentler.
If your apoB is low, your imaging is clean, and your lifetime burden is modest, no statin of any kind probably earns a place. The conversation is over before red yeast rice comes up.
This is where the beni-koji story comes to a closed loop. The Japanese deaths were a regulatory failure in a sister product. They are a reminder that "supplement" and "natural" are categories of marketing, not categories of safety. The four questions look past those categories and ask what the bottle actually contains, what it does, what it interacts with, and whether the people it was studied in look like you.
If the four questions give you a clear answer for red yeast rice, probably the most studied and most evidence-supported supplement in this category, they will give you a sharper answer for everything else on the shelf next to it.
Q&A
Is monacolin K really the same molecule as lovastatin?
Yes, structurally and pharmacologically identical. Lovastatin was originally isolated from Aspergillus terreus, and is the same compound that Monascus purpureus produces during rice fermentation. There is no chemical or biological difference. The original isolation of monacolin K and its identification as a HMG-CoA reductase inhibitor was published in 1980 [2], seven years before the FDA approved lovastatin as a prescription drug under the brand name Mevacor.
If red yeast rice contains a statin, why is it not regulated as one?
In China, it is: Xuezhikang is licensed as a drug. In the United States, the FDA classifies high-monacolin red yeast rice products as unapproved drugs, but enforcement against supplement marketers is inconsistent, and most products on US shelves contain low or undeclared monacolin K. In the European Union, food law and pharmaceutical law treat the same compound differently depending on what claim is being made and what the label states. The 2018 EFSA opinion and the subsequent 3 mg/day cap [3] closed part of the gap but left products below the threshold to continue marketing without medicines regulation.
I cannot tolerate prescription statins. Is red yeast rice a real option?
The evidence here is suggestive but limited. Several small trials have enrolled patients with documented statin intolerance and shown that they tolerate red yeast rice better, while still achieving meaningful LDL reduction of around 20% to 30% [17]; [18]. The "tolerance paradox" is incompletely understood. It may reflect lower effective dose, slower absorption, the product matrix, or a placebo effect because the patient does not realise the supplement is a statin.
What is citrinin and how do I know if it is in my product?
Citrinin is a fungal toxin (mycotoxin) that Monascus moulds can produce under suboptimal fermentation conditions. It damages the kidneys at sufficient doses. Reputable manufacturers test for and certify "citrinin-free" or "below detectable limits." If the label does not mention citrinin testing, you have no way to know. This is the kind of question that a regulated drug would not require a consumer to ask.
Why did the EU cap monacolin K at less than 3 mg per day?
EFSA's 2018 opinion concluded that the safety of monacolin K above approximately 3 mg/day could not be established for the general population, because the safety profile begins to approach that of a prescription statin at higher doses, and supplement users are typically unmonitored. The cap is a public-health pragmatic response to weak product oversight rather than a statement that 3 mg is biologically meaningful. Below the cap, the lipid effect is real but small, on the order of 10% to 15% LDL reduction rather than 25% to 35%.
Beni-koji deaths happened in Japan with a different product. Why does it matter for someone buying red yeast rice in the UK or US?
It matters because the same underlying problem (industrial fermentation of a fungus to produce a bioactive compound, sold as a supplement with weak regulatory oversight of both the active and contaminant chemistry) applies to the Western products. The specific nephrotoxin in beni-koji has not yet been identified, and case reports of acute kidney injury and Fanconi syndrome have appeared from related Kobayashi-distributed Monascus-fermented products as well [19]; [20]. The signal is not yet clear, but the principle is: a category of products that requires this much trust in unverified processes invites this kind of failure.
What is the full list of drugs that should not be combined with red yeast rice?
Beyond the three covered in the main piece (other statins, clarithromycin and other potent blockers of the drug-breakdown enzyme CYP3A4, and significant grapefruit juice intake), the documented absolute contraindications include the immunosuppressant cyclosporine in transplant patients [11]; the cholesterol drug gemfibrozil and other drugs in the fibrate class [9]; HIV regimens that contain ritonavir as a booster; the prostate-cancer drug abiraterone [12]; the antifungal medicines itraconazole and ketoconazole (a class called azoles); the antidepressant nefazodone; and any other potent blocker of the CYP3A4 enzyme. The principle to apply: anything that meaningfully blocks CYP3A4 raises monacolin K blood levels, and the risk profile becomes that of a high-dose statin in a patient without monitoring.
Should I add a CoQ10 supplement if I take red yeast rice?
The mechanistic argument is that blocking the cholesterol-production enzyme (HMG-CoA reductase) also lowers the body's own production of coenzyme Q10, which may contribute to statin-related muscle symptoms in some patients. The clinical trial evidence that CoQ10 supplementation prevents or treats statin-associated muscle symptoms is mixed and, on the most recent meta-analysis, does not show a significant benefit [21]. It is reasonable in patients with persistent muscle symptoms and unlikely to cause harm. It is not necessary for the average user.
Can I take red yeast rice in pregnancy?
No. Statins are contraindicated in pregnancy because of theoretical risk to foetal development. The same applies to red yeast rice. Anyone planning pregnancy, pregnant, or breastfeeding should not take it.
Does berberine, bergamot, or a Mediterranean diet do the same thing more safely?
Berberine and bergamot have lipid-lowering signals in smaller trials, with weaker outcome evidence than red yeast rice. The Mediterranean dietary pattern has the strongest outcome evidence of any lifestyle intervention for cardiovascular prevention, demonstrated most clearly in the PREDIMED trial [22], with no equivalent in supplement form. The ideal order of interventions for borderline-risk patients is: diet, body composition, exercise pattern, sleep, and only then a pharmacological agent.
Further Reading
[1] A. Chikasue, K. Taguchi, R. Iwatani, K. Kimura, S. Okuda, N. Uesugi, and K. Fukami, 'Three Cases of Red Yeast Rice-Containing Supplement-Induced Acute Kidney Injury and Fanconi Syndrome', Am. J. Kidney Dis., vol. 85, no. 4, pp. 522-526, Apr. 2025, doi: 10.1053/j.ajkd.2024.08.007. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/39424254/
[2] A. Endo, 'Monacolin K, a new hypocholesterolemic agent that specifically inhibits 3-hydroxy-3-methylglutaryl coenzyme A reductase', J. Antibiot. (Tokyo), vol. 33, no. 3, pp. 334-336, Mar. 1980, doi: 10.7164/antibiotics.33.334. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/7380744/
[3] EFSA Panel on Food Additives and Nutrient Sources added to Food (ANS), 'Scientific opinion on the safety of monacolins in red yeast rice', EFSA J., vol. 16, no. 8, p. e05368, Aug. 2018, doi: 10.2903/j.efsa.2018.5368. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/32626016/
[4] European Commission, 'Commission Regulation (EU) 2022/860 of 1 June 2022 amending Annex III to Regulation (EC) No 1925/2006 of the European Parliament and of the Council as regards monacolins from red yeast rice', Jun. 2022. [Online]. Available: https://eur-lex.europa.eu/legal-content/EN/TXT/?uri=CELEX:32022R0860
[5] L. Childress, A. Gay, A. Zargar, and M. K. Ito, 'Review of red yeast rice content and current Food and Drug Administration oversight', J. Clin. Lipidol., vol. 7, no. 2, pp. 117-122, Mar.-Apr. 2013, doi: 10.1016/j.jacl.2012.09.003. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/23415430/
[6] P. A. Cohen, B. Avula, and I. A. Khan, 'Variability in strength of red yeast rice supplements purchased from mainstream retailers', Eur. J. Prev. Cardiol., vol. 24, no. 13, pp. 1431-1434, Sep. 2017, doi: 10.1177/2047487317715714. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/28641460/
[7] P. Rahmani, E. Melekoglu, S. Tavakoli, N. Malekpour Alamdari, P. Rohani, and M. H. Sohouli, 'Impact of red yeast rice supplementation on lipid profile: a systematic review and meta-analysis of randomized-controlled trials', Expert Rev. Clin. Pharmacol., vol. 16, no. 1, pp. 73-81, Jan. 2023, doi: 10.1080/17512433.2023.2138342. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/36259545/
[8] Z. Lu, W. Kou, B. Du, Y. Wu, S. Zhao, O. A. Brusco et al., 'Effect of Xuezhikang, an extract from red yeast Chinese rice, on coronary events in a Chinese population with previous myocardial infarction', Am. J. Cardiol., vol. 101, no. 12, pp. 1689-1693, Jun. 2008, doi: 10.1016/j.amjcard.2008.02.056. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/18549841/
[9] C. H. Chen, Y. S. Uang, S. T. Wang, J. C. Yang, and C. J. Lin, 'Interaction between red yeast rice and CYP450 enzymes/P-glycoprotein and its implication for the clinical pharmacokinetics of lovastatin', Evid. Based Complement. Alternat. Med., vol. 2012, p. 127043, Nov. 2012, doi: 10.1155/2012/127043. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/23227093/
[10] T. Kantola, K. T. Kivistö, and P. J. Neuvonen, 'Grapefruit juice greatly increases serum concentrations of lovastatin and lovastatin acid', Clin. Pharmacol. Ther., vol. 63, no. 4, pp. 397-402, Apr. 1998, doi: 10.1016/S0009-9236(98)90034-0. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/9585793/
[11] G. V. Prasad, T. Wong, G. Meliton, and S. Bhaloo, 'Rhabdomyolysis due to red yeast rice (Monascus purpureus) in a renal transplant recipient', Transplantation, vol. 74, no. 8, pp. 1200-1201, Oct. 2002, doi: 10.1097/00007890-200210270-00028. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/12438974/
[12] Y. H. Wang, S. S. Zhang, H. T. Li, H. W. Zhi, and H. Y. Wu, 'Rhabdomyolysis-induced acute kidney injury after administration of a red yeast rice supplement: A case report', World J. Clin. Cases, vol. 11, no. 23, pp. 5547-5553, Aug. 2023, doi: 10.12998/wjcc.v11.i23.5547. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/37637685/
[13] F. Fogacci, M. Banach, D. P. Mikhailidis, E. Bruckert, P. P. Toth, G. F. Watts et al., 'Safety of red yeast rice supplementation: A systematic review and meta-analysis of randomized controlled trials', Pharmacol. Res., vol. 143, pp. 1-16, May 2019, doi: 10.1016/j.phrs.2019.02.028. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/30844537/
[14] M. Banach, N. Katsiki, G. Latkovskis, M. Rizzo, D. Pella, P. E. Penson et al., 'Postmarketing nutrivigilance safety profile: a line of dietary food supplements containing red yeast rice for dyslipidemia', Arch. Med. Sci., vol. 17, no. 4, pp. 856-863, Mar. 2021, doi: 10.5114/aoms/133716. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/34336013/
[15] A. D. Sniderman, G. Thanassoulis, T. Glavinovic, A. M. Navar, M. Pencina, A. Catapano, and B. A. Ference, 'Apolipoprotein B Particles and Cardiovascular Disease: A Narrative Review', JAMA Cardiol., vol. 4, no. 12, pp. 1287-1295, Dec. 2019, doi: 10.1001/jamacardio.2019.3780. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/31642874/
[16] B. A. Ference, H. N. Ginsberg, I. Graham, K. K. Ray, C. J. Packard, E. Bruckert et al., 'Low-density lipoproteins cause atherosclerotic cardiovascular disease. 1. Evidence from genetic, epidemiologic, and clinical studies. A consensus statement from the European Atherosclerosis Society Consensus Panel', Eur. Heart J., vol. 38, no. 32, pp. 2459-2472, Aug. 2017, doi: 10.1093/eurheartj/ehx144. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/28444290/
[17] D. J. Becker, R. Y. Gordon, S. C. Halbert, B. French, P. B. Morris, and D. J. Rader, 'Red yeast rice for dyslipidemia in statin-intolerant patients: a randomized trial', Ann. Intern. Med., vol. 150, no. 12, pp. 830-839, Jun. 2009, doi: 10.7326/0003-4819-150-12-200906160-00006. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/19528562/
[18] S. C. Halbert, B. French, R. Y. Gordon, J. T. Farrar, K. Schmitz, P. B. Morris et al., 'Tolerability of red yeast rice (2,400 mg twice daily) versus pravastatin (20 mg twice daily) in patients with previous statin intolerance', Am. J. Cardiol., vol. 105, no. 2, pp. 198-204, Jan. 2010, doi: 10.1016/j.amjcard.2009.08.672. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/20102918/
[19] K. Oda, T. Murata, F. Tanaka, H. Oda, K. Tsujimoto, A. Fukumori et al., 'A case of acute kidney injury and Fanconi syndrome while taking multiple supplements, including Red Yeast Rice Cholesterol Help®', CEN Case Rep., vol. 14, no. 1, pp. 47-51, Feb. 2025, doi: 10.1007/s13730-024-00903-0. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/38900361/
[20] Y. Katayama, R. Miyazaki, Y. Takahashi, T. Kawamura, N. Tsuboi, and T. Yokoo, 'Recurrent acute kidney injury with Fanconi syndrome related to red yeast rice supplement', CEN Case Rep., vol. 14, no. 2, pp. 178-182, Apr. 2025, doi: 10.1007/s13730-024-00926-7. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/39180649/
[21] M. Banach, C. Serban, A. Sahebkar, S. Ursoniu, J. Rysz, P. Muntner et al., 'Effects of coenzyme Q10 on statin-induced myopathy: a meta-analysis of randomized controlled trials', Mayo Clin. Proc., vol. 90, no. 1, pp. 24-34, Jan. 2015, doi: 10.1016/j.mayocp.2014.08.021. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/25440725/
[22] R. Estruch, E. Ros, J. Salas-Salvadó, M. I. Covas, D. Corella, F. Arós et al., 'Primary Prevention of Cardiovascular Disease with a Mediterranean Diet Supplemented with Extra-Virgin Olive Oil or Nuts', N. Engl. J. Med., vol. 378, no. 25, p. e34, Jun. 2018, doi: 10.1056/NEJMoa1800389. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/29897866/