
Retatrutide the wonder drug: What's Established, What's Plausible, What's Still a Hypothesis
How to look at the retatrutide data without confusing weight loss data for the cardiovascular, kidney, or cognitive benefits.
The headline
On Thursday 21 May 2026, Eli Lilly announced that participants in TRIUMPH-1, the first Phase 3 trial of retatrutide in obesity, lost an average of 28.3% of their body weight at 80 weeks on the 12 mg dose, with 45.3% losing at least 30% of their starting weight [1]. Within hours the figure was being framed as the largest sustained pharmacological weight loss yet recorded, comparable to bariatric surgery.
That number is real. It is also one number, from one indication, from one trial. Retatrutide has been studied in at least eight different conditions, and what we know about each is significantly uneven. Treating the molecule as a single story misses what the trials actually say.
For some conditions, the evidence is now strong: large, late-stage human trials (Phase 3, the kind regulators require before approving a drug) agree with the smaller, earlier trials that preceded them (Phase 2). For others, the drug improves the kind of test results doctors watch as early warning signs of disease (blood pressure, cholesterol, kidney markers), but the trials that would tell us whether the things we actually care about (heart attacks, strokes, kidney failure) also improve have not yet been reported. And for a few conditions, the only evidence is a single study in rats. Understanding those differences helps avoid misunderstanding the current status of the evidence.
The Mechanism in sixty seconds
Retatrutide activates three different receptors the body uses to control appetite, blood sugar, and energy balance. Two of them (GLP-1 and GIP) are already targets for approved drugs: GLP-1 alone for semaglutide (Ozempic, Wegovy), GLP-1 and GIP together for tirzepatide (Mounjaro, Zepbound). The third (the glucagon receptor) is new at this stage of clinical development.
Each receptor contributes something different.
GLP-1 activation slows stomach emptying and increases the feeling of fullness.
GIP activation boosts insulin release after meals and improves how fat cells handle sugar and fats.
Glucagon activation raises the rate at which the liver burns fat and increases the energy your body uses at rest.
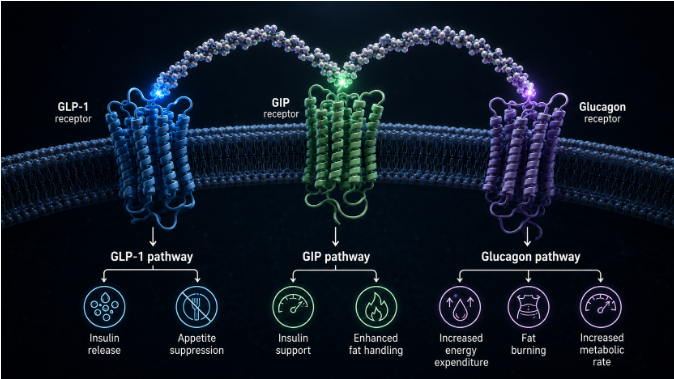
The combination of all three (triple agonism) is the design hypothesis: act on appetite, insulin, and energy burn together, with the molecule tuned to be roughly nine times more active at the GIP receptor than the body's own GIP hormone, and somewhat less strongly active at the other two [2].
High-resolution structural images of retatrutide bound to each of the three receptors, published in 2024, confirmed that one peptide can dock into three different receptor sites, providing the physical basis for the triple-receptor approach [3].
The mechanism itself is not settled. Interestingly, a separate drug currently in late-stage development, MariTide (maridebart cafraglutide), is built on the opposite premise: blocking the GIP receptor rather than activating it. In its Phase 2 trial in 592 adults with obesity, MariTide produced average weight loss of 12.3% to 16.2% at 52 weeks depending on dose, versus 2.5% with placebo [4]. Both trials were led by the same investigator, Ania Jastreboff, who also led the retatrutide Phase 2 obesity trial. One drug switches the GIP receptor on; the other switches it off; both produce large, clinically meaningful weight loss in human trials. Which approach is right, or whether each suits a different patient group, is an open question the field will not resolve quickly.
Tiered Evidence:
Tier 1 - what the trials actually show
ObesityThe strongest evidence is in obesity. The preceding Phase 2 trial enrolled 338 adults with a body mass index of at least 30 (or 27 with a weight-related condition) and ran for 48 weeks. The 12 mg dose produced a mean weight reduction of 24.2%, with 26% of participants losing 30% or more of their body weight [5]. This latest trial, TRIUMPH-1, then took 2,339 adults to the Phase 3 stage and extended follow-up to 80 weeks, with an extension to 104 weeks in higher-BMI participants. The mean weight loss reached 28.3% at 80 weeks and 30.3% at 104 weeks in the higher-BMI cohort [1].
ArthritisA separate Phase 3 trial, TRIUMPH-4, paired weight loss with knee osteoarthritis. 445 adults with obesity and symptomatic knee osteoarthritis taking 12 mg lost an average of 28.7% of body weight over 68 weeks. Pain scores on the standard knee-osteoarthritis outcome measure (the WOMAC pain subscale) fell by an average of 4.5 points, around 75.8%. About 1 in 8 participants on retatrutide were knee-pain-free at trial end [6]; [7].
Fatty liverThe next-strongest signal we're seeing is in the liver. A planned part of the Phase 2 obesity trial looked at 98 participants who also had metabolic dysfunction-associated steatotic liver disease (MASLD, the condition formerly called non-alcoholic fatty liver disease). At 24 weeks, liver-fat content (measured by non-invasive imaging, MRI-PDFF) fell by 81.4% on 8 mg and 82.4% on 12 mg, compared with a small increase in those participants on the placebo. 86% of participants on 12 mg achieved a liver fat content below 5%, which is the threshold for normal [8]. This is the largest pharmacological liver-fat effect reported in any clinical trial to date.

Blood sugar controlNot surprisingly, blood sugar control also features strongly in the evidence base. Again, a Phase 2 trial, recruiting patients with type 2 diabetes, randomised 281 adults to retatrutide, to a comparison drug that is already used in diabetes clinics (dulaglutide, a once-weekly drug that activates only one of retatrutide's three target receptors), or to a dummy injection (placebo) over 36 weeks. The 12 mg dose lowered the standard blood-sugar control marker (HbA1c) by approximately 2.0 percentage points at 24 weeks, exceeding dulaglutide's roughly 1.4 percentage point reduction. No-one experienced dangerously low blood sugar (severe hypoglycaemia), despite the addition of glucagon-receptor activation to the insulin-boosting effect of the other two receptors [9].
These are all large, humans studies with consistent directions of effect, and Phase 3 corroboration of Phase 2 findings (for weight loss and knee osteoarthritis). What they still lack is only expected at this stage, the durability of data beyond two years, and head-to-head outcome comparisons against semaglutide (Wegovy) and tirzepatide (Mounjaro).
Tier 2 - plausible but unproven
The evidence for cardiovascular and kidney benefits are one layer down. In both cases, retatrutide has been shown to positively impact the test results that doctors will track as early warning signs of disease. The trials that would then tell us whether the real-world events that matter (ie heart attacks, strokes, kidney failure) have not yet been reported.
On the heart and circulation, the Phase 2 data show consistent reductions in resting blood pressure of approximately 5 to 8 mmHg at the higher doses, alongside large improvements in the cholesterol pattern most associated with heart disease. Blood fats (triglycerides) fell by around 40%. The standard marker for harmful cholesterol-particle number (apolipoprotein-B, or apoB) fell by around 24%. Non-HDL cholesterol, which is total cholesterol minus the so-called "good" HDL fraction, fell by around 27% at 48 weeks [5]. A mechanistic study published in 2025 traced these changes substantially to a glucagon-driven reduction in a liver protein complex (ANGPTL3/8) that controls how the bloodstream clears triglycerides, a pathway most other cholesterol drugs do not target directly [10].
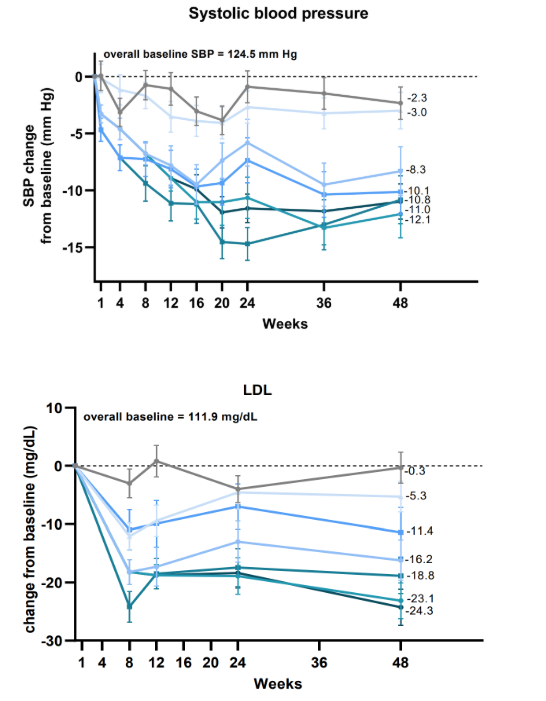
Source: [5]
Against this, resting heart rate rises by 5 to 10 beats per minute, consistent with the known class effect of GLP-1 receptor agonists [5]. No excess of clinical cardiovascular events appeared in Phase 2, but Phase 2 was not designed or powered to detect them. The dedicated cardiovascular outcomes trial (TRIUMPH-Outcomes), enrolling around 10,000 participants with established cardiovascular disease, chronic kidney disease, or high CV risk, is not expected to report until 2027 at the earliest [11].
Until then, every encouraging surrogate number comes with the same caveat: improvements in blood pressure, cholesterol, and triglycerides do not always translate to fewer real-world events. The same trials are also the only window onto long-term safety: what are the implications of the elevated resting heart-rate in patients with heart failure or irregular heartbeats, let alone healthy individuals considering the longer term health implications of these drugs. Similarly, whether a single case of pancreatitis recorded in the Phase 2 obesity trial [5] is noise or a genuine signal, and whether the muscle loss that comes with weight loss in this drug family carries consequences that only emerge over years.
On the kidneys, a pooled analysis of Phase 2 obesity and type 2 diabetes data showed reductions in the standard kidney-injury marker (the urine albumin-to-creatinine ratio, or UACR) of approximately 37% in adults with type 2 diabetes and 31.5% in adults with obesity but no type 2 diabetes, both on the 12 mg dose [12]. Kidney function markers stayed stable or improved. Whether this translates into protection against the events that matter (kidney failure, dialysis) remains to be tested. No dedicated kidney-outcomes trial of the kind semaglutide ran has yet been registered for retatrutide.
Tier 3 - the frontier
Three possible use cases are in the territory where the evidence base barely exists. The right framing here is that something is plausible via the biological mechanism and has not yet been demonstrated in humans, at a systems level.
The first is cognition.
The broad argument for this class of drugs in conditions affecting memory and thinking is reasonable. GLP-1 receptor agonists reduce inflammation in the brain and the protein-deposit changes characteristic of Alzheimer's disease in animal models, and early-stage clinical trials of older drugs in the same class have produced suggestions of preservation of cognitive function in mild memory and thinking problems and in Parkinson's disease, although large-scale confirmation is still not there [13]; [14]. The cognition-specific retatrutide human data is currently zero.
The only retatrutide-specific cognitive evidence in any species is a 2026 preprint reporting that, in male rats with chemically induced diabetes, retatrutide preserved spatial learning and short-term memory, reduced one inflammation-driving chemical (TNF-alpha) in the brain's memory centre (the hippocampus), and partially protected the surface layer of the brain (the cortex) and the hippocampus from the damage seen in untreated diabetic rats [15]. That is the entire dataset. There is no Phase 2 or Phase 3 trial of retatrutide for cognitive outcomes registered in the public domain currently.
The second is obstructive sleep apnoea (the condition in which the upper airway repeatedly collapses during sleep and interrupts breathing, closely associated with obesity). A sub-study running inside the Phase 3 weight-loss trials is studying retatrutide in adults with obesity and moderate-to-severe sleep apnoea, but no results are available [7].
The third is liver histology. The strong evidence showing an 82% reduction in liver fat in those with MASLD is profound, but the further question, whether retatrutide actually resolves any of the underlying inflammation and scarring of the liver has not been studied. Other drugs in the broader liver-disease pipeline have shown that improvements in liver fat and improvements in fibrosis can actually be separate. In the most directly relevant comparator with semaglutide, MASH resolution was achieved in 62.9% of patients on the drug while fibrosis improvement reached only 36.8%, leaving substantially less overlap than the headline numbers might imply [16].
What to watch and what to do
The next 18 months will substantially redraw this picture. Three further Phase 3 trial results in the TRIUMPH programme are due before the end of 2026: TRIUMPH-2 in obesity with type 2 diabetes, TRIUMPH-3 in obesity with established cardiovascular disease (with further safety information relevant to higher-risk populations), and obstructive sleep apnoea. TRANSCEND-T2D-2, a head-to-head comparison against semaglutide, has completed enrolment and is now following participants [17]. The cardiovascular outcomes trial reports late 2027 or 2028. If retatrutide follows the typical regulatory pathway, a first approval for obesity could arrive in 2026 or 2027.
Three practical takeaways
First, decide whether you actually need to act now or can wait. If you don't have obesity and/or significant complications, the answer may well be that waiting is reasonable. The most important unknowns (cardiovascular safety, evidence on hard kidney outcomes, head-to-head tirals etc) all report between now and 2028. If you already have established cardiovascular disease, advanced kidney disease, or significant fatty liver disease, the calculation changes. That is a conversation worth having frankly with your doctor.
Second, if you do go on retatrutide or any drug in this family, plan resistance training and adequate protein intake from day one. Around 20-25% of the weight lost on these drugs is muscle and bone rather than fat [18]. The mitigation is well-established and unglamorous: lift weights, eat enough protein. Your doctor will write the prescription but the commitment to a strength training programme is with you.
Third, when retatrutide becomes available and you start seeing claims about it, the question to ask your doctor is not "does it work?" but "for my specific situation, what does it improve that we already know about, and what hasn't been studied yet?" Weight, blood-sugar control, and liver fat sit on strong evidence. Heart attacks, strokes, kidney failure, brain health, and sleep apnoea claims do not yet.
Q&A
Is retatrutide just a stronger Ozempic?
It is in the same family of drugs (incretin-based pharmacotherapy for weight and metabolic disease) but it acts on three receptors rather than one. Semaglutide, the active ingredient in Ozempic and Wegovy, activates only the GLP-1 receptor. Tirzepatide (Mounjaro, Zepbound) activates two: GLP-1 and GIP. Retatrutide activates all three: GLP-1, GIP, and glucagon. The third receptor changes the metabolic profile in ways the other drugs cannot reproduce, particularly for liver fat and triglyceride handling. Whether that translates to a better overall outcome at the level of cardiovascular events, kidney protection, or long-term function is not yet known. Head-to-head trials against semaglutide are recruiting and have not been reported.
Does retatrutide prevent heart attacks or strokes?
There is no current evidence that retatrutide reduces cardiovascular events. The biomarker changes (lower blood pressure, better lipid profile) are favourable and create a reasonable prior expectation, but the dedicated cardiovascular outcomes trial (TRIUMPH-Outcomes) is not expected to report until late 2027 or early 2028. Until then, any claim that retatrutide reduces heart attacks, strokes, or cardiovascular death goes beyond what the data support.
There is also a separate safety question, distinct from efficacy: retatrutide raises resting heart rate by 5 to 10 beats per minute, which has not yet been characterised in patients who already have heart failure or irregular heartbeats. If that describes you, this is worth flagging explicitly to your doctor before any treatment decision.
Will it help with brain fog, cognitive decline, or dementia?
Not on current evidence. The only retatrutide-specific cognitive study is a 2026 preprint in rats with chemically induced diabetes. There are no human cognitive trials. The class-level case for GLP-1 receptor agonists in cognitive disease is mechanistically plausible but is awaiting Phase 3 trials to confirm. Any claim for retatrutide being good for brain health is currently reasoning from a hypothesis, not from human data.
Will I lose muscle on it?
Around 20-25% of the weight lost on retatrutide is muscle and bone rather than fat, similar to other drugs in this family. This matters more in older adults, in anyone whose function depends on strength, and in anyone with low muscle reserve to start with. The mitigation is well-established and unglamorous: lift weights, eat enough protein.
When will retatrutide be available?
As of May 2026 it is not approved anywhere. Eli Lilly has signalled intent to file with the FDA in the United States and the EMA in Europe after the TRIUMPH-1, 2, and 3 readouts. First approvals for obesity are anticipated in 2026 or 2027 if the regulatory submissions are accepted.
Further Reading
[1] Eli Lilly and Company, 'Lilly's triple agonist, retatrutide, delivered powerful weight loss in pivotal Phase 3 obesity trial', Investor press release, May 2026. [Online]. Available: https://investor.lilly.com/news-releases/news-release-details/lillys-triple-agonist-retatrutide-delivered-powerful-weight-loss
[2] T. Coskun et al., 'LY3437943, a novel triple glucagon, GIP, and GLP-1 receptor agonist for glycemic control and weight loss: from discovery to clinical proof of concept', Cell Metab., vol. 34, no. 9, pp. 1234-1247.e9, Sep. 2022, doi: 10.1016/j.cmet.2022.07.013.
[3] W. Li, Q. Zhou, Z. Cong, et al., 'Structural insights into the triple agonism at GLP-1R, GIPR and GCGR manifested by retatrutide', Cell Discov., vol. 10, no. 1, p. 77, Jul. 2024, doi: 10.1038/s41421-024-00700-0.
[4] A. M. Jastreboff, D. H. Ryan, H. E. Bays, P. R. Ebeling, M. G. Mackowski, N. Philipose, et al., 'Once-Monthly Maridebart Cafraglutide for the Treatment of Obesity - A Phase 2 Trial', N. Engl. J. Med., vol. 393, no. 9, pp. 843-857, Sep. 2025, doi: 10.1056/NEJMoa2504214.
[5] A. M. Jastreboff, L. M. Kaplan, J. P. Frías, et al., 'Triple-Hormone-Receptor Agonist Retatrutide for Obesity - A Phase 2 Trial', N. Engl. J. Med., vol. 389, no. 6, pp. 514-526, Aug. 2023, doi: 10.1056/NEJMoa2301972.
[6] Eli Lilly and Company, 'Lilly's triple agonist, retatrutide, delivered weight loss of up to an average of 71.2 lbs along with substantial relief from osteoarthritis pain in first successful Phase 3 trial', Investor press release, Dec. 2025. [Online]. Available: https://investor.lilly.com/news-releases/news-release-details/lillys-triple-agonist-retatrutide-delivered-weight-loss-average
[7] G. Giblin et al., 'Retatrutide for the treatment of obesity, obstructive sleep apnea and knee osteoarthritis: Rationale and design of the TRIUMPH registrational clinical trials', Diabetes Obes. Metab., vol. 28, no. 1, pp. 83-93, Jan. 2026, doi: 10.1111/dom.70209.
[8] A. J. Sanyal, L. M. Kaplan, J. P. Frias, et al., 'Triple hormone receptor agonist retatrutide for metabolic dysfunction-associated steatotic liver disease: a randomized phase 2a trial', Nat. Med., vol. 30, no. 7, pp. 2037-2048, Jul. 2024, doi: 10.1038/s41591-024-03018-2.
[9] J. Rosenstock, J. Frias, A. M. Jastreboff, et al., 'Retatrutide, a GIP, GLP-1 and glucagon receptor agonist, for people with type 2 diabetes: a randomised, double-blind, placebo and active-controlled, parallel-group, phase 2 trial conducted in the USA', Lancet, vol. 402, no. 10401, pp. 529-544, Aug. 2023, doi: 10.1016/S0140-6736(23)01053-X.
[10] Y. Wen, D. Lemen, Y. Lin, et al., 'Decreases in circulating ANGPTL3/8 concentrations following retatrutide treatment parallel reductions in serum lipids', Diabetes Obes. Metab., vol. 27, no. 10, pp. 5985-5995, Oct. 2025, doi: 10.1111/dom.16661.
[11] Eli Lilly and Company, 'The Effect of Retatrutide Once Weekly on Cardiovascular Outcomes and Kidney Outcomes in Adults Living With Obesity (TRIUMPH-Outcomes)', ClinicalTrials.gov identifier NCT06383390. [Online]. Available: https://clinicaltrials.gov/study/NCT06383390
[12] H. J. L. Heerspink, Z. Lu, Y. Du, et al., 'The Effect of Retatrutide on Kidney Parameters in Participants With Type 2 Diabetes Mellitus and/or Obesity', Kidney Int. Rep., vol. 10, no. 6, pp. 1980-1992, Jun. 2025, doi: 10.1016/j.ekir.2025.03.049.
[13] A. Roy, V. L. Dawson, and T. M. Dawson, 'From metabolism to mind: The expanding role of the GLP-1 receptor in neurotherapeutics', Neurotherapeutics, vol. 22, no. 5, p. e00712, Sep. 2025, doi: 10.1016/j.neurot.2025.e00712.
[14] M. Urkon, E. Ferencz, J. A. Szász, et al., 'Antidiabetic GLP-1 Receptor Agonists Have Neuroprotective Properties in Experimental Animal Models of Alzheimer's Disease', Pharmaceuticals, vol. 18, no. 5, p. 614, May 2025, doi: 10.3390/ph18050614.
[15] U. Keskin, E. Altın, M. K. Kara, et al., 'Effects of Retatrutide on Learning and Memory in Streptozotocin-Induced Diabetic Rats', bioRxiv, Jan. 2026 (revised Apr. 2026), doi: 10.64898/2026.01.23.701347. [Online]. Available: https://www.biorxiv.org/content/10.64898/2026.01.23.701347v2
[16] A. J. Sanyal, P. N. Newsome, I. Kliers, et al., 'Phase 3 Trial of Semaglutide in Metabolic Dysfunction-Associated Steatohepatitis', N. Engl. J. Med., vol. 392, no. 21, pp. 2089-2099, Jun. 2025, doi: 10.1056/NEJMoa2413258.
[17] Eli Lilly and Company, 'Effect of Retatrutide Compared With Semaglutide in Adult Participants With Type 2 Diabetes and Inadequate Glycemic Control With Metformin With or Without SGLT2 Inhibitor (TRANSCEND-T2D-2)', ClinicalTrials.gov identifier NCT06260722. [Online]. Available: https://clinicaltrials.gov/study/NCT06260722
[18] T. Coskun, Q. Wu, N. C. Schloot, et al., 'Effects of retatrutide on body composition in people with type 2 diabetes: a substudy of a phase 2, double-blind, parallel-group, placebo-controlled, randomised trial', Lancet Diabetes Endocrinol., vol. 13, no. 8, pp. 674-684, Aug. 2025, doi: 10.1016/S2213-8587(25)00092-0.