
Does fish oil actually speed up training recovery? The evidence for omega-3 in recovery, and the dose worth trialling if you decide to.
The gap between the marker and the feeling
A 2026 meta-analysis bringing together 41 randomised controlled trials found that omega-3 supplementation reduces several markers of exercise-induced inflammation and muscle damage, with moderate effect sizes [1]. On its own, that seems like a clear case for adding fish oil to a hard training block. The problem is that the headline finding and the effect you actually care about are not the same thing. Lower interleukin-6 (IL-6; a marker of inflammation) on a blood draw is a clear biochemical result. Recovering faster, being able to train again sooner, or feeling less wrecked the next day is an outcome. The two are related, but they are not interchangeable, and the gap between them is what we need to understand.
Omega-3 is no substitute for sleep, adequate protein, or sensible load management, and it is not a direct, reliable performance enhancer. Those remain the foundation. It is a small, low-risk lever on top of them: any edge is modest and works mostly through recovery, not a direct boost to output.
What the evidence actually says
Across all the 41 trials together, the effect is real. The 2026 meta-analysis reported moderate reductions in IL-6, tumour necrosis factor-alpha (TNF-alpha; another marker of inflammation), creatine kinase (CK; an enzyme that leaks into the blood when muscle is damaged), and delayed-onset muscle soreness (DOMS; the stiffness and ache that builds a day or two after hard exercise), with effect sizes of roughly -0.4 to -0.7 on a common statistical scale (standardised mean differences, where about -0.5 counts as a moderate effect) [1]. That includes muscle soreness itself, not only the blood markers. The strongest effects appeared in recreational rather than elite athletes.
A small controlled human trial suggests similar findings. In 11 adults supplemented for one week, soreness after eccentric arm exercise (muscle-lengthening contractions, the kind that reliably cause next-day ache) rose by about 15% less than in the control condition [2].
So, on average, across many trials, omega-3 supplementation suggests a moderate reduction in both inflammatory markers and perceived soreness after demanding exercise. For a cheap, low-risk supplement, that is a meaningful and worthwhile effect.
Why individual results vary
The difficulty is that the average hides a lot of disagreement between individual trials, and some individual trials find the blood marker effect without a clear change in how people feel or perform.
In one randomised trial of 20 men, fish oil lowered markers of cell-level wear from hard exercise (oxidative stress), including thiobarbituric acid reactive substances (TBARS; a marker of fat being oxidised in the blood) and DNA's susceptibility to oxidative damage in a lab challenge, but produced no difference in CK, muscle soreness, or maximal voluntary contraction (MVC; the most force a muscle can produce in one all-out effort) [3]. The biology shifted. How the participants felt and how their muscles performed did not.
This is the recurring pattern worth remembering: a marker can move without the desired function following.
A separate meta-analysis of 12 randomised trials found that omega-3 did produce a statistically significant reduction in DOMS, but the effect was smaller than the threshold usually considered clinically meaningful, and muscle strength and range of motion did not improve [4].
The study designs lets the data down. A systematic evaluation of omega-3 trials in physically trained participants concluded that no study met all recommended design standards, that doses and durations varied widely, and that concerns about flaws in how the trials were run (risk of bias) were common enough to make firm recommendations difficult [5]. The overall effect seems to be real, but the trials behind it vary in quality so view the effect as probable rather than proven, though not a reason to dismiss it.
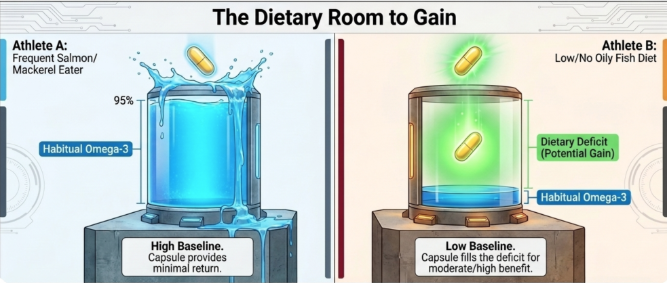
There is one practical refinement. The effect is more plausible if your habitual diet is low in oily fish. Someone already eating salmon or mackerel several times a week has less obvious room to gain from a capsule than someone whose baseline intake is minimal.
A reasonable dose to challenge the effect
If you decide to trial it, the dose that carried the strongest effects in the meta-analysis was at least 2 g/day of combined eicosapentaenoic acid and docosahexaenoic acid (EPA and DHA; the two active long-chain omega-3 fats in fish oil), taken for a minimum of six weeks [1]. The International Society of Sports Nutrition position paper likewise treats omega-3 as a supplement with a justifiable role in recovery and adaptation [6]. Shorter than 6 weeks or lower-dose attempts are unlikely to show much of an effect.
The same consensus paper also points to benefits beyond just recovery: omega-3 can have a beneficial influence on immune-cell responses in athletes, is associated with better sleep quality, and, taken regularly, may offer some neuroprotection for those exposed to repeated head impacts [6]. These effects are, however, still currently more tentative than the DOMS data, but for a low-risk supplement they add to the case for at least a trial to assess any benefits on an individual level.
As with any supplement, always discuss these with your own doctor, they are not a fully benign intervention. A meta-analysis of 81,210 participants in cardiovascular outcome trials found that marine omega-3 supplementation was associated with an increased risk of atrial fibrillation (AF; an irregular, often rapid heart rhythm), with a clear dose relationship: the risk was raised by roughly 12% at doses up to 1 g/day and by roughly 49% above 1 g/day (hazard ratios of about 1.12 and 1.49) [7].
A larger, more recent analysis puts that signal in context. After analysing 34 trials and 114,326 people, it found the extra AF risk was essentially confined to one group: older people already at high cardiovascular risk taking high doses (above about 1.5 g/day), where the odds of AF rose by roughly half (odds ratio 1.48), an absolute increase of less than 1%. At lower doses, and in people not already at high cardiovascular risk, no clear increase in the rates of AF appeared, even at higher intakes [8]. Remember though, this is one preprint, and two of its authors have commercial omega-3 interests, so it should be treated as suggestive rather than a settled evidence base.
In sum, for a young, healthy, low-cardiovascular-risk person taking around 2 g/day, the AF risk is likely small and may not apply at all. It is a more material consideration for an older individual, or anyone with cardiac history or AF risk factors, especially at higher doses.
What the evidence points to in practice
For anyone who has talked it through with their own doctor and been given no reason to avoid fish oil, a few practical points come out of the evidence.
First, the doses that actually moved the needle were around 2 g/day of combined EPA and DHA, taken with a meal, for at least six weeks. Shorter durations or smaller doses might not have the same or any effect.
Second, a sensible interpretation looks at function and soreness across a training block, not the feeling of being "less inflamed" or a requirement to look at specific blood markers to know if it is working.
Third, the evidence does not support pushing past 2 to 3 g/day for bigger gains, and the AF risk rises with dose, most clearly in people already at cardiovascular risk. That makes higher doses questionable for older readers, or anyone with cardiac history, and something to discuss with their doctor.
Fourth, it sits behind sleep, protein, and load management, not ahead of them. If those are not handled, a fish oil capsule is not the magic lever that changes recovery.
Q&A
Will fish oil speed up my recovery?On average, across many trials, supplementation suggests a moderate reduction in soreness and inflammatory markers after hard exercise [1]. But individual trials disagree, and some find the marker change without any soreness or performance benefit [3]. One meta-analysis judged the soreness reduction real but too small to be clinically meaningful, with no gain in strength or range of motion [4]. Treat it as a small possible help, not a reliable accelerator.
What dose and for how long?The strongest effects in the pooled data came from at least 2 g/day of combined EPA and DHA for a minimum of six weeks, taken with food [1]. Shorter trials are unlikely to tell you anything useful.
Is more better?No. The evidence does not support escalating the dose for bigger recovery gains, and higher intakes carry a rising risk of atrial fibrillation, concentrated in people already at cardiovascular risk [7], [8]. More is not a free upgrade.
Capsules or oily fish?Diet first. The benefit from a supplement is more plausible if your habitual oily fish intake is low; if you already eat it several times a week, the additional gain from capsules is less clear.
Is it safe?At these doses it is generally well tolerated. The main caution is a dose-related signal for atrial fibrillation, and a larger, more recent analysis suggests this sits mostly with older people already at cardiovascular risk taking high doses, with little or no signal in low-risk people [7], [8]. If you are considering trialling this, discuss this with your doctor, especially if you have established or cardiac risk factors.
Further Reading
[1] Z. Li and B. Zhang, 'Effects of omega-3 supplementation on inflammation and recovery in sports: a meta-analysis', FASEB J., vol. 40, no. 7, Art. no. e71709, Apr. 2026, doi: 10.1096/fj.202504783R.
[2] K. B. Jouris, J. L. McDaniel, and E. P. Weiss, 'The effect of omega-3 fatty acid supplementation on the inflammatory response to eccentric strength exercise', J. Sports Sci. Med., vol. 10, no. 3, pp. 432-438, Sep. 2011. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/24150614/
[3] P. Gray, A. Chappell, A. M. Jenkinson, F. Thies, and S. R. Gray, 'Fish oil supplementation reduces markers of oxidative stress but not muscle soreness after eccentric exercise', Int. J. Sport Nutr. Exerc. Metab., vol. 24, no. 2, pp. 206-214, Apr. 2014, doi: 10.1123/ijsnem.2013-0081.
[4] Z.-T. Lv, J.-M. Zhang, and W.-T. Zhu, 'Omega-3 polyunsaturated fatty acid supplementation for reducing muscle soreness after eccentric exercise: a systematic review and meta-analysis of randomized controlled trials', Biomed. Res. Int., vol. 2020, Art. no. 8062017, Apr. 2020, doi: 10.1155/2020/8062017.
[5] R. Anthony, M. J. Macartney, J. L. Heileson, P. L. McLennan, and G. E. Peoples, 'A review and evaluation of study design considerations for omega-3 fatty acid supplementation trials in physically trained participants', Nutr. Res. Rev., vol. 37, no. 1, pp. 1-13, Jun. 2024, doi: 10.1017/S095442242300001X.
[6] R. Jäger, J. L. Heileson, S. Abou Sawan, B. L. Dickerson, M. Leonard, R. B. Kreider, et al., 'International Society of Sports Nutrition position stand: long-chain omega-3 polyunsaturated fatty acids', J. Int. Soc. Sports Nutr., vol. 22, no. 1, Art. no. 2441775, Dec. 2025, doi: 10.1080/15502783.2024.2441775.
[7] B. Gencer, L. Djoussé, O. T. Al-Ramady, N. R. Cook, J. E. Manson, and C. M. Albert, 'Effect of long-term marine omega-3 fatty acids supplementation on the risk of atrial fibrillation in randomized controlled trials of cardiovascular outcomes: a systematic review and meta-analysis', Circulation, vol. 144, no. 25, pp. 1981-1990, Dec. 2021, doi: 10.1161/CIRCULATIONAHA.121.055654.
[8] N. R. Abuknesha, J. H. O'Keefe, F. Qian, N. L. Tintle, Y. Lin, Y. Sun, et al., 'Effects of omega-3 fatty acid treatment on risk for atrial fibrillation: an updated meta-analysis of 34 trials including 114,326 individuals', medRxiv, Dec. 2025, doi: 10.64898/2025.12.14.25342167. [Online]. Available: https://pubmed.ncbi.nlm.nih.gov/41445624/