
TB-500 Is Not the Peptide You Think It Is: Most marketing borrows evidence from a different molecule. Here is how to tell.

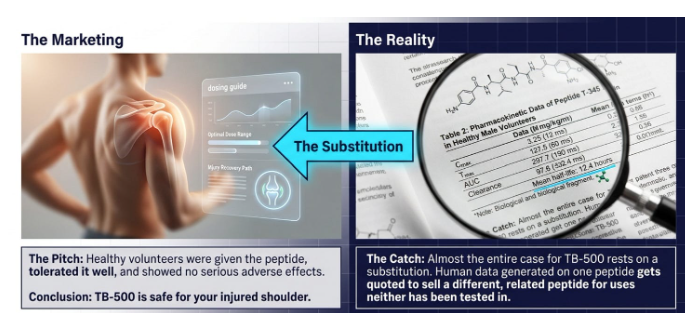
Not an unusual scenario. Someone forwards me a study, or a social-media post that might cite one, or a polished clinical guide with dosing tables and a credentialed name on the cover. Healthy volunteers were given thymosin β4 by infusion, tolerated it well, and showed no serious adverse effects. The implication being: TB-500 is safe, so it is worth a try for a shoulder or a tendon that will not settle.
The data is genuine. The problem is that the molecule in those studies is not the molecule sold as TB-500.
Almost the entire case for TB-500 rests on that substitution. Human data generated on one peptide gets quoted to sell a different, related peptide for uses neither has been tested in. Once you understand that, most of the marketing becomes flawed.
A word on what this piece is not. It is not a claim that peptide therapeutics as a class are worthless. They are a genuinely interesting area of medicine. It is a narrower argument: that this compound, sold this way, now, is running a long way ahead of its evidence, and that the confusion between the two molecules is much of what makes that possible.
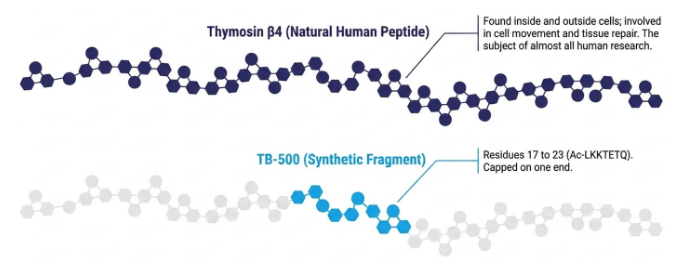
TB-500 is not thymosin β4
Here is the distinction the market depends on you not noticing.Thymosin β4 is a natural human peptide. It is a chain of 43 amino acids found inside and outside cells, with a role in cell movement and tissue repair. Almost all of the human research worth citing was done on this full-length peptide, or on a lab-made copy of it.TB-500 is not that. In anti-doping and analytical chemistry work, TB-500 is described as a short synthetic fragment: a seven-amino-acid stretch from the middle of thymosin β4 (residues 17 to 23, written Ac-LKKTETQ), with a chemical cap on one end [1].A fragment is exactly what it sounds like. It is a piece of the parent molecule, not the whole thing. Sharing a sequence with thymosin β4 does not make TB-500 interchangeable with it, any more than a single page proves the contents of a book. Whether the fragment reproduces any clinically meaningful part of the parent peptide’s biology in humans is, at present, an open question rather than an established fact.
There is a plain reason the fragment, not the full peptide, is what gets sold. A seven-amino-acid chain is cheap and simple to synthesise as a research chemical, whereas a clean 43-amino-acid peptide is harder and costs more to make; the fragment also covers the region of thymosin β4 often described as its active part, which lets sellers argue you only need that piece. That argument assumes the one thing not yet shown: that the isolated fragment behaves like the parent in humans.
You do not have to take my word for the distinction. The one human trial registered specifically on the marketed compound calls it, in its own title, the “Thymosin Beta 4 17-23 Fragment”. It is a Phase I/II study in adults with stable cardiovascular disease, currently recruiting, with no results posted [2]. The people studying TB-500 formally are careful to name it as a fragment. The people selling it tend not to be.
What has actually been tested in humans
Strip the claims back to the human evidence and a narrow, specific picture appears. Importantly, nearly all of it is on full-length thymosin β4, not on TB-500.
The clearest signal is in eye disease. In a small Phase III trial in neurotrophic keratopathy (a condition where the cornea loses sensation and fails to heal), complete healing at four weeks occurred in 6 of 10 patients on thymosin β4 eye drops versus 1 of 8 on placebo [3]. That reads well, but it is worth understanding the detail: the comparison did not reach statistical significance on the primary measure (p = 0.0656), the trial enrolled 18 people, and two of the authors were employed by the company developing the product. Earlier dry-eye trials of the same eye-drop formulation showed a similar pattern: some improvement in signs and symptoms in a 9-patient study [4], and a larger 72-subject trial that was mixed rather than cleanly positive [5].
On safety, two early-phase studies gave full-length or lab-made thymosin β4 by infusion to healthy volunteers and reported no dose-limiting toxicity and no serious adverse events over short exposures [6][7]. Useful, but limited: these were short courses, by drip, in supervised settings, with no test of whether the peptide does anything for recovery or performance.
Notice what is absent. There is no human trial showing that thymosin β4, let alone the TB-500 fragment, heals a tendon, repairs a muscle, speeds recovery, or improves performance in healthy people.
The strongest human evidence sits in eye disease, in a specific drop formulation, and it does not transfer to a syringe aimed at a shoulder.
The tendon promise, and the “Wolverine stack”
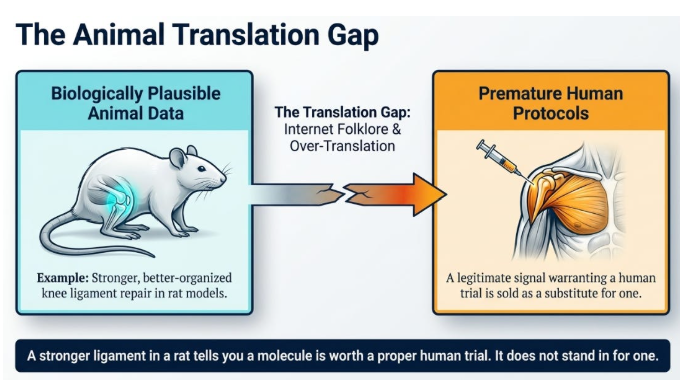
So where do the tendon and muscle claims come from? Almost entirely from animals.
Thymosin β4 has improved healing in animal injury models. In one rat study, it produced better-organised, stronger repair of a knee ligament [8]. There is also a wound-healing literature in animals, and a small human signal in leg ulcers with a topical gel [9]. This is the legitimate basis for scientific interest, and it is biologically plausible. It is also exactly the kind of finding that gets over-translated online. A stronger ligament in a rat tells you a molecule is worth a proper human trial. It does not stand in for one
The combination claim is weaker still. TB-500 is increasingly sold paired with BPC-157, marketed as a “Wolverine stack” for accelerated repair. On the direct evidence, the position is pretty blunt: there is no published human trial of the two together, no combination toxicology, and no convincing indexed animal study showing the pair outperforms either peptide alone. The rationale is an extrapolation from two separate preclinical stories, stitched together by marketing and community folklore.
Combining two experimental peptides does not average their uncertainty. It compounds it. The accurate description is not synergy. It is stacked uncertainty, with a product-quality risk that doubles rather than halves. For the wider evidence base on BPC-157 specifically, I have written separately about the difference between an evidence gap and a cover-up.
Reading the regulatory tea leaves
Three regulatory facts get misread, each in a way that flatters the product.
First, the FDA story. You may have heard that the FDA is “legalising” peptides. It is not. For 23 to 24 July 2026, the FDA has scheduled an advisory committee meeting to discuss whether several nominated substances, including TB-500-related and BPC-157-related compounds, should be considered for a compounding list [10]. Advisory committees give non-binding recommendations. A meeting to discuss eligibility for compounding is not an approval, and the FDA separately lists substances of this kind as potentially presenting significant safety risks [11].
Second, the UK position. In April 2026 the medicines regulator opened an investigation into peptide clinics making health claims about products they cannot legally sell as medicines [12]. The label “research use only” does not neutralise this. A product marketed with therapeutic claims can fall inside medicines law regardless of what the vial says.
Third, anti-doping. Thymosin β4 and its derivatives, including TB-500, are prohibited at all times under the WADA growth-factor section, and BPC-157 is prohibited as a non-approved substance [13]. “Undetectable” is not a safe inference, and for any tested athlete it is the wrong question. Prohibited is prohibited.
The misreading travels in respectable company, which is what makes it hard to spot. I have seen peptide guides, written by genuinely well-credentialed specialists and laid out with dosing tables, monitoring schedules and certificate-of-analysis language, tell readers that TB-500 is “not listed” for sport and that athletes need only arrange “individual review”. It is prohibited at all times [13].
The polish of a document, and the standing of whoever wrote it, are not evidence that its claims are right. They are the reason people trust a claim before checking it out.
Underneath all three quietly sits a larger problem: what is actually in the vial. Anti-doping analysis has found products sold as TB-500 that were misbranded or were not the labelled compound at all [1]. With a grey-market, self-injected product, identity and sterility are not assumptions you get to make for free.
How not to get caught by the next one
This will not be the last peptide marketed to you on borrowed evidence. So the useful output is not to give you a verdict on one compound, but a test you can reuse in future too.
Two concrete moves, both doable before you part with any money.
First, separate the molecule from the marketing, then ask for proof of identity. Establish whether the product is the full-length peptide that was actually studied or a fragment that was not, and ask the seller for a certificate of analysis and independent third-party assay confirming what the vial contains and that it is sterile. If they cannot produce one, you are not evaluating a therapy. You are buying a complete unknown, not even a research molecule.
Second, if you compete in any tested sport, make WADA status the first filter, not the last. Check the prohibited list before anything else [13]. For TB-500 and BPC-157 it ends the conversation.
And the deeper filter, the one that survives the next product too: who funded the human evidence, what population was it in, and where does it sit on the evidence hierarchy, from case report up to controlled trial. If the answers are looking thin, the molecule is at the same stage of maturity as TB-500, however good the rat data look.
The foundations have not moved. For tendons, muscle, and recovery, the things with actual human evidence remain unglamorous: progressive loading, sleep, protein, managed training load, time. A fragment of a peptide, named after the whole, sold on someone else’s trial, is not yet a reason to abandon them. There are also better evidenced emerging therapeutics for specific injuries in specific circumstances.
Q&A
Are TB-500 and thymosin β4 the same thing?No, and this is the central confusion. Thymosin β4 is the full 43-amino-acid natural peptide. TB-500, as sold and as described in anti-doping chemistry, is a short fragment of it (residues 17 to 23) [1]. Most human research is on the full peptide, so quoting it as proof for the fragment is not evidence-based.
Is there any good human evidence for thymosin β4 at all?Some, but it is narrow and formulation-specific. The clearest signals are in eye disease using a drop formulation, such as neurotrophic keratopathy and dry eye [3][4], plus short-term infusion safety data in healthy volunteers [6]. None of it supports injecting TB-500 for recovery or performance.
Does the TB-500 and BPC-157 combination work better than either alone?There is no human trial, no combination safety study, and no convincing animal study of the pair [2]. The synergy claim is currently unsupported by direct evidence and is best described as stacked uncertainty.
Doesn’t the FDA’s July 2026 meeting mean these peptides are being approved?No. It is an advisory committee meeting to discuss whether certain substances should be considered for a compounding list, and such committees issue non-binding recommendations [10]. A discussion about eligibility for compounding is not a product approval.
Further Reading
[1] World Anti-Doping Agency, ‘Investigation of in vitro/ex vivo TB-500 metabolism and synthesis of relevant metabolites’, WADA Scientific Research Projects. [Online]. Available: https://www.wada-ama.org/en/resources/scientific-research/investigation-vitroex-vivo-tb-500-metabolism-synthesis-relevant
[2] ‘TB-500 (Thymosin Beta 4 17-23 Fragment) for Cardiovascular Biomarkers in Stable ASCVD’, ClinicalTrials.gov identifier NCT07487363. [Online]. Available: https://clinicaltrials.gov/study/NCT07487363
[3] G. Sosne, H. K. Kleinman, C. Springs, R. H. Gross, J. Sung, and S. Kang, ‘0.1% RGN-259 (Thymosin β4) ophthalmic solution promotes healing and improves comfort in neurotrophic keratopathy patients in a randomized, placebo-controlled, double-masked phase III clinical trial’, Int. J. Mol. Sci., vol. 24, no. 1, art. no. 554, Dec. 2022, doi: 10.3390/ijms24010554.
[4] G. Sosne, P. Dunn, and C. Khanna, ‘Thymosin β4 significantly improves signs and symptoms of severe dry eye in a phase 2 randomized trial’, Cornea, vol. 34, no. 5, pp. 491-496, May 2015, doi: 10.1097/ICO.0000000000000379.
[5] G. Sosne, H. K. Kleinman, and D. Larsen, ‘Thymosin beta 4 ophthalmic solution for dry eye: a randomized, placebo-controlled, Phase II clinical trial conducted using the controlled adverse environment (CAE) model’, Clin. Ophthalmol., vol. 9, pp. 877-884, 2015, doi: 10.2147/OPTH.S80954.
[6] D. Ruff, G. Crockford, G. Girardi, and Y. Zhang, ‘A randomized, placebo-controlled, single and multiple dose study of intravenous thymosin beta4 in healthy volunteers’, Ann. N. Y. Acad. Sci., vol. 1194, pp. 223-229, Apr. 2010, doi: 10.1111/j.1749-6632.2010.05474.x.
[7] X. Wang et al., ‘A first-in-human, randomized, double-blind, single- and multiple-dose, phase I study of recombinant human thymosin β4 in healthy Chinese volunteers’, J. Cell. Mol. Med., vol. 25, no. 17, pp. 8222-8228, Sep. 2021, doi: 10.1111/jcmm.16693.
[8] B. Xu, X. Yang, and Z. Yan, ‘Thymosin β4 enhances the healing of medial collateral ligament injury in rat’, Regul. Pept., vol. 184, pp. 1-5, Jun. 2013, doi: 10.1016/j.regpep.2013.03.026.
[9] G. Guarnera, A. DeRosa, and R. Camerini, ‘The effect of thymosin treatment of venous ulcers’, Ann. N. Y. Acad. Sci., vol. 1194, pp. 207-212, Apr. 2010, doi: 10.1111/j.1749-6632.2010.05490.x.
[10] U.S. Food and Drug Administration, ‘July 23-24, 2026 meeting of the Pharmacy Compounding Advisory Committee’. [Online]. Available: https://www.fda.gov/advisory-committees/advisory-committee-calendar/july-23-24-2026-meeting-pharmacy-compounding-advisory-committee-07232026
[11] U.S. Food and Drug Administration, ‘Certain bulk drug substances for use in compounding that may present significant safety risks’. [Online]. Available: https://www.fda.gov/drugs/human-drug-compounding/certain-bulk-drug-substances-use-compounding-may-present-significant-safety-risks
[12] The Guardian, ‘Medicines watchdog to investigate UK peptide clinics over health claims’, Apr. 2026. [Online]. Available: https://www.theguardian.com/society/2026/apr/04/medicines-watchdog-to-investigate-uk-peptide-clinics-over-health-claims
[13] World Anti-Doping Agency, ‘The Prohibited List’. [Online]. Available: https://www.wada-ama.org/en/prohibited-list