
Fibre for women: a simple change to live longer?

A signal worth noticing in postmenopausal women
Most of what we say about fibre and living longer comes from studies that pool men and women together. A 2026 analysis of US national survey data did something less common: it looked specifically at postmenopausal women, 7,708 of them, followed for up to two decades [1].
The headline is the kind that hits home. Women in the highest third of fibre intake had a lower rate of death over follow-up than women in the lowest third, with all-cause mortality about 15% lower and cardiovascular mortality about 31% lower [1]. Across 2,116 deaths, of which 657 were cardiovascular, that is a sizeable gap.
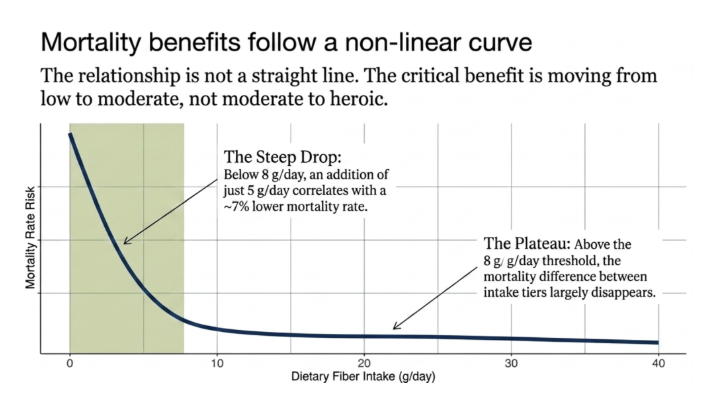
Two things are worth saying before anyone overdoes it on the fibre supplements. This is an association, not a demonstrated cause. And the relationship was not a straight line: the benefit was concentrated at the lower end of intake. Below roughly 8 g/day, women who ate 5 g/day more had about a 7% lower mortality rate, while above that level the difference largely disappeared [1].
The interesting movement is from low to moderate, not moderate to heroic.
The broader picture agrees on direction
A women-only finding is more convincing when it sits within a wider body of evidence pointing the same way, and here it does.
The most complete synthesis to date pooled 64 prospective cohorts and more than 3.5 million people [2]. Comparing the highest fibre intakes with the lowest, all-cause mortality was 23% lower and cardiovascular mortality 26% lower. Insoluble fibre, the kind in whole grains and vegetable skins, showed a stronger association than soluble fibre.
So the direction is consistent. Higher habitual fibre intake is associated with lower mortality across very large populations, and the postmenopausal finding fits that pattern rather than being contrary to the main evidence base.
Where the women-specific evidence is thinner
A consistent direction across mostly mixed-sex data is not the same as a settled answer in women. The female-specific evidence is thinner than the headline suggests, and the one large cohort that looked directly at fibre and fatal cardiovascular disease in women did not fall in line.
The UK Women's Cohort followed 31,036 women [3]. For total fibre, it found no significant protective association: the hazard ratio was 0.91 per 6 g/day, with a confidence interval that crossed 1, which is compatible with no effect. The only signal that survived was narrow, a lower fatal stroke risk from cereal fibre in overweight women specifically.
That null finding is less of a contradiction than it first looks, because the two studies were not measuring the same thing in the same people. The UK cohort estimated fibre from food-frequency questionnaires in a younger, health-conscious sample (mean age 52, not specifically postmenopausal) with a narrow intake range and only 258 fatal cardiovascular events, which leaves little contrast to detect [3]. The US analysis used 24-hour recall in older postmenopausal women across a wider social range, with more cardiovascular deaths to work with [1]. Different assessment tool, different population, different power.
That exception does not overturn the direction. It sets how much confidence the headline deserves, and leads to the two considerations that should frame how this is read.
Two considerations that keep this real
The first is what fibre actually is in the data. It is a marker of a dietary pattern, not an isolated input. The 2026 American Heart Association guidance makes the same point from the other direction: cardiovascular benefit comes from a whole pattern built on vegetables, fruit, whole grains and legumes, with minimally processed foods over ultra-processed ones [4].
Fibre is a feature of that pattern, not a nutrient to bolt on to an otherwise poor diet.
The second consideration is measurement. The postmenopausal finding rests on self-reported 24-hour dietary recall, a method with well-documented random and systematic error, including energy under-reporting and day-to-day variation that a single recall cannot capture [5]. That does not invalidate the result. It does mean the precise gram thresholds should be read as directional, not as a target to hit to the decimal.
What to actually do with this
The practical implications are:
First, get fibre from whole foods spread across the day rather than from a supplement: a vegetable portion, a whole grain, or a serving of legumes at each main meal. The non-linear curve in the postmenopausal data suggests the association concentrates in the move from a low intake to a moderate one, so if your baseline is low, this is the change with the most signal behind it [1].
Second, judge the pattern, not the number. Build meals around vegetables and fruit, whole grains and legumes, minimally processed [4], and let fibre follow from that. Chasing a fibre count with bran sachets on top of an otherwise refined diet is not what these cohorts were measuring.

In summary, in postmenopausal women, higher fibre intake is associated with lower all-cause and cardiovascular mortality, the broad evidence agrees on direction, but at least one large women's cohort does not. Treat fibre as one reliable feature of a good dietary pattern, worth prioritising if your intake is low, and not as a mortality lever in its own right.
Q&A
Does eating more fibre make postmenopausal women live longer?The data show an association, not proof of cause. Women with higher fibre intake had lower all-cause and cardiovascular mortality in a US postmenopausal cohort [1], and the same direction appears across 3.5 million people [2]. But fibre intake tracks with overall diet quality and lifestyle, so part of the apparent benefit may belong to those companions rather than to fibre itself.
How much fibre is the point of diminishing returns?In the postmenopausal data, the association was concentrated at low intakes: below roughly 8 g/day, women who ate 5 g/day more had about 7% lower mortality, while above that level the difference largely disappeared [1]. Read that as directional. The numbers come from self-reported recall, which carries real measurement error [5].
Why did a large women's cohort find no benefit?The UK Women's Cohort found no significant association between total fibre and fatal cardiovascular disease, only a narrow signal for cereal fibre and stroke in overweight women [3]. The likeliest reason is methodological rather than a real reversal: it estimated fibre from food-frequency questionnaires in a younger, health-conscious sample (mean age 52, not specifically postmenopausal) with few cardiovascular deaths to work with, leaving little contrast to detect. The broad direction across the larger evidence still points one way, so this is one thin-data exception, not a field in conflict.
Is a fibre supplement as good as fibre from food?The evidence here was built on dietary fibre from whole foods, and cardiovascular guidance frames benefit at the level of a whole dietary pattern, not a single added nutrient [4]. Adding a supplement to an otherwise poor diet is not what these studies measured, and the evidence does not support treating it as equivalent.
Further Reading
[1] Y. Guo, M. Li, and W. Zhuang, 'Association of dietary fiber intake with all-cause and cardiovascular mortality in postmenopausal U.S. women: A NHANES 1999-2018 cohort study', Maturitas, vol. 203, p. 108752, Dec. 2025, doi: 10.1016/j.maturitas.2025.108752.
[2] F. Ramezani, F. Pourghazi, M. Eslami, M. Gholami, N. Mohammadian Khonsari, H. S. Ejtahed, et al., 'Dietary fiber intake and all-cause and cause-specific mortality: An updated systematic review and meta-analysis of prospective cohort studies', Clin. Nutr., vol. 43, no. 1, pp. 65-83, Jan. 2024, doi: 10.1016/j.clnu.2023.11.005.
[3] D. E. Threapleton, D. C. Greenwood, V. J. Burley, M. Aldwairji, and J. E. Cade, 'Dietary fibre and cardiovascular disease mortality in the UK Women's Cohort Study', Eur. J. Epidemiol., vol. 28, no. 4, pp. 335-346, Apr. 2013, doi: 10.1007/s10654-013-9799-6.
[4] A. H. Lichtenstein, A. Khera, C. A. M. Anderson, L. J. Appel, D. M. DeSilva, C. Gardner, et al., '2026 Dietary Guidance to Improve Cardiovascular Health: A Scientific Statement From the American Heart Association', Circulation, Mar. 2026, doi: 10.1161/CIR.0000000000001435.
[5] R. S. Gibson, U. R. Charrondiere, and W. Bell, 'Measurement Errors in Dietary Assessment Using Self-Reported 24-Hour Recalls in Low-Income Countries and Strategies for Their Prevention', Adv. Nutr., vol. 8, no. 6, pp. 980-991, Nov. 2017, doi: 10.3945/an.117.016980.