
Does eating late actually raise cardiovascular risk, or does it just correlate with other risk behaviours?
As a clinician who also thinks about food and training a lot, we hear a lot about the influence of late night meals on sleep quality.
But people often ask a simple question.
Does eating late affect also real health outcomes, like cardiovascular risk, or does it only affect sleep.
The quick answer is that no one study can tell you what to do, but emerging research gives us clues. A large French cohort looked closely at the timing of meals to see how it relates to cardiovascular risk [1].
This large French cohort demonstrated modest increases in risk with later first meals and later last meals.The data do not prove causation, though they do suggest that timing interacts with circadian biology in ways worth taking seriously.
Firstly, to make sense of the results, it helps to understand why timing of meals is even a question.
Why timing might matter
Our bodies follow daily rhythms. Circadian biology means that the brain and peripheral tissue, such as cells in the musculoskeletal system, the cardiovascular system and other bodily systems, run on their own clocks [2]. These clocks influence heart rate, blood pressure and metabolism.
When our eating schedule falls out of step with these rhythms, the balance between the sympathetic and parasympathetic nervous systems can shift. That provides a plausible link between late meals and cardiovascular strain, but direct causal evidence in humans is limited.
Most data are observational, and trials tend to be short and focused on risk markers rather than cardiovascular events.
Meal timing as a circadian cue
Meal timing is not just a behavioural marker. It is one of the cues that helps synchronise peripheral clocks across tissues [3]. Food timing can cause metabolic clocks to drift away from the light and sleep cycle, creating internal circadian misalignment even when sleep or morning light exposure is consistent.
The NutriNet‑Santé study
In this study, researchers followed 103 389 adults in France who provided repeated 24‑hour dietary records over several years. They calculated when people first ate, when they finished eating, how many “eating occasions” they had and how long they fasted overnight. After a median of 7.2 years of follow-up, there were 2 036 new cases of cardiovascular disease.
Delaying the first meal by one hour was associated with a 6% higher risk of cardiovascular disease. Having the last meal after 9 PM, compared with before 8 PM, was linked to a 13% higher risk.
When the researchers looked specifically at stroke and transient ischaemic attack, each hour delay in the last meal increased risk by 8%, and eating after 9 PM raised risk by 28%.
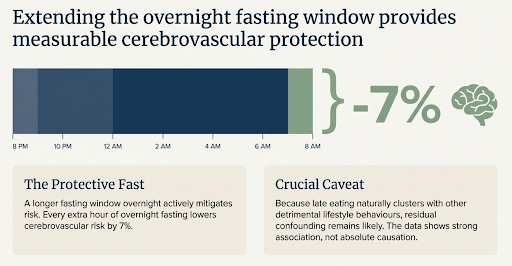
A longer fasting window overnight appeared protective: every extra hour of fasting lowered cerebrovascular risk by 7%. The number of eating occasions did not matter for cardiovascular outcomes. Notably, the associations were stronger in women than in men. Residual confounding remains likely, because late eating clusters with other behaviours.
Consistency with other prospective evidence
Two other cohort studies help put these observations in perspective. In a cohort of 26 902 male health professionals from the United States, skipping breakfast was associated with a 27% higher risk of coronary heart disease, and late‑night eating was linked to a 55% increase [4]. In a large meta‑analysis pooling more than two million participants, breakfast skipping was associated with increased risks of cardiovascular disease, coronary artery disease, stroke and cardiovascular mortality [5].
Skipping Breakfast
Breakfast skipping in cohort studies is not the same thing as a structured time restricted plan. In real life, many people who “skip breakfast” simply start later and also finish later. That can shorten the overnight fast and push more eating into the biological evening. It is a different exposure from a deliberate pattern that ends earlier and protects the overnight fasting window.
Randomised trials help separate the impact of timing from calories. In a controlled feeding crossover trial where calories were kept high enough to maintain the same weight across the trial, an earlier time restricted feeding window still improved insulin sensitivity and blood pressure, suggesting an effect not explained by weight loss alone [6].
In contrast, a 16:8 pattern that effectively pushes eating later in the day did not outperform consistent meal timing in the TREAT trial [7]. That is why “time restricted eating” should be seen as a spectrum, not a single, defined intervention. Some versions may work mainly by helping to reduce calories (if you simply cannot fit more calories in within a specific window), some may benefit from earlier timing, and in most people it is probably both.
Generalisability and different populations
Meal‑timing behaviours vary across cultures. A cross‑sectional analysis of 8 147 Korean adults found that those who consumed more of their daily energy in the evening had higher odds of obesity and metabolic syndrome [8]. In a Japanese cohort followed for nineteen years, people who skipped breakfast had higher risks of cardiovascular and coronary heart disease mortality [9]. These studies do not prove causation, but they add strength to the argument that late eating and breakfast omission correlate with metabolic and cardiovascular risks across diverse populations. Differences in diet composition, meal size and lifestyle may modulate the effect, so one size will never fit all.
Mechanistic and safety considerations
Mechanisms remain speculative. Circadian misalignment can influence autonomic balance, and late meals may interfere with overnight repair processes. Time‑restricted eating, which extends the overnight fast, has shown promise in small trials. A recent paper summarised these trials, noting that restricting eating to a smaller daily window lowered body weight and blood pressure, improved blood glucose, insulin sensitivity, and did not lead to serious adverse events [10]. Mild side effects such as headaches and fatigue were noted. The evidence base is still young, so more long‑term studies are needed.
Key takeaways
If you are considering meal timing as part of a prevention strategy, several points stand out.
Eating earlier in the day and extending the overnight fast may reduce cardiovascular risk, especially for stroke.
Skipping breakfast and eating late at night have been associated with higher coronary heart disease risk in other cohorts. These patterns also align with studies showing higher risks of cardiovascular events and mortality among breakfast skippers.
Extending the overnight fasting window via time‑restricted eating appears safe in the short term and may improve metabolic markers, but evidence is limited. Any fasting regimen should be personalised and balanced with overall dietary quality and energy needs.
Keep the foundations solid: diet quality, activity, sleep, blood pressure, lipids, and smoking status explain far more cardiovascular risk than meal timing alone.

These findings sit atop decades of research showing that diet quality, physical activity, sleep and traditional risk factor management drive cardiovascular health. Meal timing may be one lever among many. For most people, choosing eating times that support stable energy, good sleep and consistent adherence will be more important than chasing a particular hour on the clock.
Q and A
Does eating late actually raise cardiovascular risk, or does it just correlate with other risk behaviours?
The most honest answer is that the cohort data cannot prove cause. In NutriNet Santé, later first meals and later last meals were associated with higher cardiovascular risk, and longer overnight fasting was associated with lower cerebrovascular risk, but residual confounding is likely because meal timing clusters with sleep timing, alcohol, activity patterns, social factors, and diet quality [1]. What the study adds is that the signal persists after multivariable adjustment, and it is stronger for cerebrovascular outcomes than for coronary heart disease [1].How big is the effect, really?
Modest. In NutriNet Santé, each hour delay in the first meal was associated with HR 1.06 for overall cardiovascular disease. For cerebrovascular disease, each hour delay in the last meal was HR 1.08, and eating after 9 pm versus before 8 pm was HR 1.28 [1]. These are not “order of magnitude” effects. They sit in the range where confounding can still matter.Is this mainly about sleep quality?
Sleep is a plausible pathway, but the NutriNet Santé analysis is about cardiovascular events, not sleep outcomes [1]. The bigger point is that sleep and meal timing are tightly linked in real life. That makes it hard to isolate one from the other without controlled studies.Why treat meal timing as more than a behavioural marker?
Because meal timing is a circadian cue. A controlled laboratory study showed that shifting meal timing can shift metabolic rhythms even when core circadian markers such as melatonin do not move in the same way, which is a practical definition of internal misalignment [3]. That supports the claim that “late eating” can be physiologically meaningful, not just a label for lifestyle chaos.Why might the associations look stronger in women?
The study reports stronger associations in women than men [1]. That could reflect biology, behaviour, baseline risk, or measurement differences. Without a mechanism test or a trial stratified by sex, we should treat this as a consistent subgroup observation, not an explanation.If breakfast skipping correlates with risk, should everyone eat breakfast?
Not automatically. Cohort “breakfast skipping” often means a later first meal and sometimes a later last meal, which can shorten the overnight fast. That is not the same exposure as a deliberate time restricted pattern that ends earlier. The US cohort linked breakfast skipping with higher coronary heart disease risk, and late night eating with an even larger increase [4]. A meta analysis also found higher risks across cardiovascular disease, coronary artery disease, stroke, and cardiovascular mortality among breakfast skippers [5]. Those are signals, not prescriptions.So is time restricted eating protective, or is it just calorie reduction?
It can be both, and the balance matters. Early time restricted feeding improved insulin sensitivity and blood pressure in a controlled feeding crossover study without weight loss, which suggests an effect beyond calorie reduction in that setting [6]. In contrast, a 16:8 window from noon to 8 pm did not outperform consistent meal timing in the TREAT trial [7]. That is why “time restricted eating” should be described as a family of patterns, not one intervention.Is there any safety signal I should worry about with time restricted eating?
A review of time restricted eating trials describes it as generally safe and feasible in the short term, with few serious adverse events reported, but mild symptoms such as headache and fatigue occur [10]. The evidence base is still dominated by short duration studies and risk markers, not long term event outcomes.
Further Reading
[1] A. Palomar-Cros et al., ‘Dietary circadian rhythms and cardiovascular disease risk in the prospective NutriNet-Santé cohort’, Nat. Commun., vol. 14, no. 1, p. 7899, Dec. 2023, doi: 10.1038/s41467-023-43444-3.
[2] I. R. Kelters, Y. Koop, M. E. Young, A. Daiber, and L. W. van Laake, ‘Circadian rhythms in cardiovascular disease’, Eur. Heart J., vol. 46, no. 36, pp. 3532–3545, Jul. 2025, doi: 10.1093/eurheartj/ehaf367.
[3] S. M. T. Wehrens et al., ‘Meal Timing Regulates the Human Circadian System’, Curr. Biol. CB, vol. 27, no. 12, pp. 1768-1775.e3, Jun. 2017, doi: 10.1016/j.cub.2017.04.059.
[4] L. E. Cahill et al., ‘Prospective study of breakfast eating and incident coronary heart disease in a cohort of male US health professionals’, Circulation, vol. 128, no. 4, pp. 337–343, Jul. 2013, doi: 10.1161/CIRCULATIONAHA.113.001474.
[5] H. Zhang, S. Zhang, Y. Liu, X. Wang, and J. Hu, ‘The association between skipping breakfast and cardiovascular disease: a meta analysis’, Front. Cardiovasc. Med., vol. 12, Dec. 2025, doi: 10.3389/fcvm.2025.1565806.
[6] E. F. Sutton, R. Beyl, K. S. Early, W. T. Cefalu, E. Ravussin, and C. M. Peterson, ‘Early Time-Restricted Feeding Improves Insulin Sensitivity, Blood Pressure, and Oxidative Stress Even without Weight Loss in Men with Prediabetes’, Cell Metab., vol. 27, no. 6, pp. 1212-1221.e3, Jun. 2018, doi: 10.1016/j.cmet.2018.04.010.
[7] D. A. Lowe et al., ‘Effects of Time-Restricted Eating on Weight Loss and Other Metabolic Parameters in Women and Men With Overweight and Obesity: The TREAT Randomized Clinical Trial’, JAMA Intern. Med., vol. 180, no. 11, pp. 1491–1499, Nov. 2020, doi: 10.1001/jamainternmed.2020.4153.
[8] S. Jeong, H. Lee, S. Jung, J. Y. Kim, and S. Park, ‘Higher energy consumption in the evening is associated with increased odds of obesity and metabolic syndrome: findings from the 2016-2018 Korea National Health and Nutrition Examination Survey (7th KNHANES)’, Epidemiol. Health, vol. 45, p. e2023087, Sep. 2023, doi: 10.4178/epih.e2023087.
[9] J. Tang et al., ‘Breakfast Type and Cardiovascular Mortality: The Japan Collaborative Cohort Study’, J. Atheroscler. Thromb., vol. 30, no. 9, pp. 1255–1264, Sep. 2023, doi: 10.5551/jat.63564.
[10] A. A. Kirkham, E. B. Parr, and A. S. Kleckner, ‘Cardiometabolic health impacts of time-restricted eating: Implications for type 2 diabetes, cancer, and cardiovascular diseases’, Curr. Opin. Clin. Nutr. Metab. Care, vol. 25, no. 6, pp. 378–387, Nov. 2022, doi: 10.1097/MCO.0000000000000867.